
Download
Bladder | 2023 | Vol. 10 | e21200005
DOI: 10.14440/bladder.2023.856
DOI: 10.14440/bladder.2023.856
REVIEW
Advances in the bladder cancer research using 3D culture models
Yexin Gu1†, Ye Lu1†, Yunqiang Xiong2†, Xiangpeng Zhan2, Taobin Liu2, Min Tang1, An Xie2, Xiaoqiang Liu2*, Bin Fu2*
1Cyberiad Intelligent Technology, Shanghai 201112, China.
2Department of Urology, the First Affiliated Hospital of Nanchang University, 17 Yongwai Street, Nanchang City, Jiangxi Province, China.
2Department of Urology, the First Affiliated Hospital of Nanchang University, 17 Yongwai Street, Nanchang City, Jiangxi Province, China.
†These authors contributed equally to this work.
*Corresponding author: Fu Bin, Department of Urology, the First Affiliated Hospital of Nanchang University, 17 Yongwai Street, Nanchang City, Jiangxi Province, China; E-mail: urofbin@163.com, Tel.: 13879103861; Xiaoqiang Liu, Department of Urology, the first affiliated Hospital of Nanchang City, Jiangxi, China; E-mail: shaw177@163.com, Tel.: 18702523942
Conflict of interest: The authors do not have any possible conflicts of interest.
Abbreviation used: 2D, two-dimensional; 3D, three-dimensional; NMIBC, Non-muscle invasive bladder cancer; MIBC, muscle-invasive bladder cancer; UICC, The Union for International Cancer Control; TURBT, Transurethral removal of bladder tumor; ADM, Adriamycin; HCPT, hydroxycamptothecin; BGC, Bacillus Calmette Guerin vaccine; GC, Gemcitabine plus cisplatin; MVAC, methotrexate, vinblastine, doxorubicin, and cisplatin; MVP, methotrexate, vinblastine, cisplatin; FANFT, n-[4-(5-nitro-2-furyl) -2-thiazolyl] formamide; BBN, N-butyl-N (4-hydroxybutyl) nitrosamine; MNU, N-methyl-N-nitrosourea; BCPN, N-butyl-N-(3-carboxypropyl) nitrosamine; DLP, digital-light processing; GelMA, gelatin methacryloyl; PDT, patient-derived μtissues
Received October 21, 2022; Revision received January 31, 2023; Accepted February 28, 2023; Published May 30, 2023
Abstract
Bladder cancer represents the most common malignancy of the urinary system, posing a significant threat to patients' life. Animal models and two-dimensional (2D) cell cultures, among other traditional models, have been used for years to study various aspects of bladder cancer. However, these methods are subject to various limitations when mimicking the tumor microenvironment in vivo, thus hindering the further improvement of bladder cancer treatments. Recently, three-dimensional (3D) culture models have attracted extensive attention since they overcome the shortcomings of their traditional counterparts. Most importantly, 3D culture models more accurately reproduce the tumor microenvironment in the human body because they can recapitulate the cell-cell and cell-extracellular matrix interactions. 3D culture models can thereby help us gain deeper insight into the bladder cancer. The 3D culture models of tumor cells can extend the culture duration and allow for co-culturing with different cell types. Study of patient-specific bladder cancer mutations and subtypes is made possible by the ability to preserve cells isolated from particular patients in 3D culture models. It will be feasible to develop customized treatments that target relevant signaling pathways or biomarkers. This article reviews the development, application, advantages, and limitations of traditional modeling systems and 3D culture models used in the study of bladder cancer and discusses the potential application of 3D culture models.
Keywords: bladder cancer, cell culture, 3D culture models, 3D bioprinting
1. Background
Bladder cancer is a malignant tumor resulting from the uncontrolled proliferation of abnormal cells in the bladder. It is one of the commonest malignant tumors of the urinary system. According to the World Health Organization, nearly 430,000 patients are diagnosed with bladder cancer and more than 165,000 died of the cancer annually [1]. An epidemiological report released in 2019 stated that the incidence rate and mortality rate of bladder cancer rank among the top ten in China [2].
Bladder cancer presents a severe threat to public health due to its high recurrence rate and mortality rate. The current "one-size-fits-all" approach is not, by many, deemed the best strategy since it does not consider the potential impact of patient-specific genetic variations on drug response. Therefore, it is essential to develop new treatments. 2D cell cultures are primarily used in basic and clinical research of drugs. Cell culture is an essential technique employed in drug development, providing a simple, rapid, and economical way. 2D cell culture is a valuable technique for cell-based research, but it has limitations. Practically, all cells in the in vivo environment are surrounded by extracellular matrix and other cells. Therefore, 2D cell culture sometimes provides unreliable data that may mis-represent in vivo responses. Currently, the standard procedure of compound screening in new drug development starts with the test based on 2D cell culture, followed by animal tests and clinical trials. Only about 10% of the tested compounds successfully move forward to clinical development, and many drugs failed clinical trials. Animal modeling was shifted to in vivo culture, but the microenvironment of allogeneic models was significantly different from that of naturally occurring tumors, and and tumor induction is time-consuming and labor-intensive. Therefore, it is essential to develop and establish in vitro cell systems that can more closely simulate the behavior of cells in vivo. 3D culture models were created as a solution to these restraints.
2. Conventional models for Bladder Cancer Studies
2.1 In vitro 2D cell Culture Models
2D cell culture refers to a technique of growing and expanding cells on a flat substrate [3], and the 2D cell culture modeling is a primary methodology for studying cell physiology and pathology in vitro. Because cells can only grow and expand in two dimensions as a single layer, they are mostly spindle-shaped and flat [4]. Cells grown in 2D usually have strong proliferation ability but poor differentiation ability. Compared with in vivo models, the expression levels of related genes and proteins in cells in 2D models tend to be very different [5,6]. Compared to 3D models, 2D cell models lack the ability to reflect the effect of the microenvironment and extracellular matrix on cells. Presently, the commonly used human cell lines of bladder cancer include UMUC-3, RT-112, RT4, and T24 [7,8], as well as common drug-resistant strains of human cell lines of bladder cancer, such as cisplatin-resistant strain T24/DDP and penicillin-resistant strain Pumc-91/ADM [9,10]. The basic data of each bladder cancer cell line, such as origin, development, molecular characteristics, culture, and preservation conditions, are available in the widely used databases listed in Table 1 [11]. However, the genomic landscape, phenotypes, and physiological activity of 2D cultured cells of bladder cancer differ from those of cells in vivo [12]. Researchers thus are now seeking more physiologically-relevant cell culture models, such as 3D culture technology with a microenvironment closer to cells in vivo.
Table 1 Online database of bladder cancer cell linesnote
| Database | Name | Resource | Website |
|---|---|---|---|
| Achilles | Genome scale RNAi and CRISPR-Cas9 silencing and knockdown of individual genes to identify genes that affect cell survival. | https://portals.broadinstitute.org/achilles | |
| BC-BET | Bladder Cancer Biomarker Evaluation Tool | Rapid evaluation of candidate gene expression across 40 commonly used human bladder cancer cell lines. | https://gdancik.github.io/bioinformatics/BCBET |
| CCLE | Cancer Cell Line Encyclopedia | Genetic characterization of human cell lines | https://portals.broadinstitute.org/ccle |
| Cellosaurus | Database for cell lines | https://web.expasy.org/cellosaurus/ | |
| COSMIC | Catalogue of Somatic Mutations in Cancer | Somatic mutations in human cancer cell lines | http://cancer.sanger.ac.uk/cosmic |
| CTRP | Cancer Therapeutics Response Portal | Identifying and targeting cancer dependencies with small molecules | https://portals.broadinstitute.org/ctrp/ |
| GDSC | Genomics of Drug Sensitivity in Cancer | Identifying molecular features of cancers that predict response to anticancer drugs | http://www.cancerrxgene.org/ |
| IARC TP53 | International Agency for Research on Cancer (IARC) TP53 Database | Compiles various types of data and information on human TP53 gene variations related to cancer | http://p53.iarc.fr/ |
| ICLAC | International Cell Line Authentication Committee | Resource lists cell lines that are currently known to be cross-contaminated or misidentified | http://iclac.org/ |
| TCPA | MD Anderson Cancer Cell Line Project | Proteomic database of cancer cell lines | http://tcpaportal.org/ |
| UC-25 | Exome sequencing of bladder cancer cell lines | http://www.synapse.org/UC25 |
2.2 Animal Models
Animal research is a crucial intermediate step between cellular experiments and clinical studies during the drug development process. Animals and humans are similar in physiological, pathological, and genetic terms, rendering the animal model an essential experimental vehicle for in vivo research. There are currently four types of animal models of bladder cancer: in situ carcinogen-induced model, in situ tumor transplantation model, ectopic tumor transplantation model, and genetically-engineered model [13].
2.2.1 In situ carcinogen-induced models
Commonly used carcinogens include n-[4-(5-nitro-2-furyl)-2-thiazolyl] formamide (FANFT), N-butyl-N (4-hydroxybutyl) nitrosamine (BBN) and N-methyl-N-nitrosourea (MNU) [14]. For the model establishment, a carcinogen, such as BBN, is dissolved into concentrations between 0.01% ‒ 0.05% in drinking water and fed to the experimental animals. The induction takes about 5‒8 months. To create a model, a drug is directly administered to the bladder mucosa through intravesical perfusion, at the doses of 2 or 2.5 mg each time, once every two weeks, and 2‒4 times per therapy, with the overall induction time lasting for roughly 8 weeks [15]. FANFT is a nitrofuran compound, and an indirect carcinogen. It plays a carcinogenic role principally through the co-oxidation of prostaglandin H synthase in bladder mucosa. It is generally given orally, together with feeding food, at a common concentration of 0.2%, and the induction taking at least 8 months [16]. These carcinogenic compounds have a long drug cycle, low specificity for tumor formation, differ from spontaneous tumors, and are very likely to kill animals. Therefore, these features make them unsuitable for the study of bladder cancer.
2.2.2 In situ tumor transplantation models
The most popular technique for making orthotopic bladder cancer models, along with the advancement of carcinogenic technologies, involves implanting bladder cancer cells into animals. It falls into two categories, i.e., homo-transplantation and xenotransplantation in terms of the source of cell lines used. The in situ transplantation model has been widely accepted for its practicality. Recently, the focus of the work has been directed to improving the success rate of modeling and transplantation techniques. However, in situ tumor transplantation models have shortcomings, such as long construction cycles, poor reproducibility, and unwanted interaction between the mouse's implanted tumor cells and host cells. Moreover, since xenotransplantation uses nude mice as hosts, it doesn't allow for the study of the immune mechanism of bladder cancer, which has posed a major limitation on the application of the current in situ bladder tumor transplantation model.
2.2.3 Ectopic tumor transplantation models
Intraperitoneal, intravenous, and subcutaneous transplantation of bladder cancer cells or tumor tissue blocks into animals are common methods to establish bladder cancer ectopic transplantation models [17,18]. These techniques are frequently used to study tumor-related mechanisms and assess the efficacy of new medications [19]. The ectopic transplantation model is a simpler and more practical approach in comparison to in situ transplantation model. However, the number of cells cannot be easily determined when tumor tissue blocks are transplanted, leading to inconsistency in tumor formation. What is more, the ectopic transplantation tumor models also have some aforementioned shortcomings of the in situ transplantation tumor model. Besides, some researchers, like Jonathan B et al. [20] found that the ectopic transplantation tumor model failed to predict the results of tumor metastasis since the tumor was not in situ.
2.2.4 Genetically-engineered model
Genetically-engineered models allow for the investigation of the mechanisms of tumor formation and the interactions between genetic background and environmental variables. A genetically-engineered model is an animal model with the target genes knocked out or incorporated by using genetic engineering technology [21]. Currently, the target genes that have been confirmed to be closely related to bladder cancer include H-Ras, p53, Rb, PTEN, fibroblast growth factor receptor, and epidermal growth factor receptor (EGFR) [22]. The first model of BC in transgenic mice used simian virus 40 (SV40) large T antigen derived from the tissue-specific mouse UPII gene promoter, which is expressed in the basal layer of the urothelium [23]. Other oncogenes, when placed under the control of UPII, have been used to generate transgenic mice model of BC, such as EGFR and H-Ras [24]. A new uroplakin II promoter (UPKII)-dependent expression vector has been created and future work will be necessary/needed to validate the same phenotype observed in the original transgenic mouse model [25]. Recent research has focused on this paradigm, but genetically-engineered models also have several limitations. The tumor derived from the genetically-engineered animal models is genetically too simple, while the development mode of actual human bladder cancer is mechanistically diverse. Moreover, the establishment cycle of animal models is long and expensive.
3. 3D culture models for bladder cancers
To build 3D culture models, multiple cell types are cultivated in vitro in physiologically relevant biomaterial scaffolds. Cells grow and proliferate in all dimensions as if in vivo, so their morphologies are more physiologically-relevant [26,27]. 3D structures can mimic the gradient of nutrient supply and metabolite clearance in the body, boost the ability of cell differentiation and proliferation, and have genes and proteins expressed at levels comparable to those of cells in vivo [21]. We herein introduced three types of promising 3D culture technologies that have been evolving fast, including organoid culture, 3D bioprinting model, and microfluidic chip model.
3.1 Organoids
The utility of organoids in the research of genetic diseases has attracted extensive attention due to the functional reproduction of organoids. Organoids are clusters of cell spheres composed of specific cells that have differentiated from stem cells. Organoids have a similar tissue spatial structure to the corresponding organs and can reproduce/mimic some functions of the original organs, thus providing an intimately related physiological system [28,29]. Suk Hyung Lee et al. [30] have established a bank of bladder cancer organoid lines from 22 patient tissue samples. Through genome mapping, researchers confirmed that the organoid lines are highly consistent with the corresponding parent tumor both histopathologically and in terms of gene mutation spectra. Drug sensitivity experiments confirmed that organoid lines with different mutation spectra respond differently to drugs, indicating that the molecular spectrum of organoids can be used to identify drug efficacy. In addition, many studies utilized drug sensitivity tests to determine the cell state of organoid culture, as shown in Table 2 [28, 30-33]. Lamy et al. [34] demonstrated, by using exon sequencing, that tumor evolution occurred in an organoid culture of bladder cancer samples without drug treatment, and the mode of development was similar to that of primary human bladder cancer. However, organoid culture technology is also confronted with some challenges, such as difficulties in achieving vascularization of the organoids and simulating the interaction between tumor organoids and immune cells in vitro, as well as the structural variability of organoids and the size difference between pluripotent cell lines. In addition, the fidelity of organoids also presents a significant challenge.
Table 2 Organoid Susceptibility Test
| References | Medicine | n | Experimentation |
|---|---|---|---|
| Suk Hyung Lee et al. [30] | Drug susceptibility test (trametinib; Gemcitabine) | 22 cases | Organoids larger than 100 μm were eliminated through cell strainers. Each well of ultra-low attachment 96-well plates was placed with 15‒20 organoids containing 2% Matrigel. Medium and drug concentrations varied from 10 μmol/L to 128 pmol/L or 100 μmol /L to 1.28 nmol/L. Cell viability was measured by CellTiter-Glo 3D (Promega) 6 days after drug administration. |
| Mohamed Elbadawy et al. [31] | Drug susceptibility test (piroxicam; gemcitabine; cisplatin; vinblastine) | Each well of 96-well plates was inoculated with 5,000 organoids, followed by addition of drugs of different concentrations [piroxicam (0.1‒10 μmol/L), gemcitabine (1‒100 nmol/L), cisplatin (0.1‒100 μmol/L] or vinblastine (0.01‒10 nmol)/L) for 3 days. The Alamar blue kit was finally used for cell viability assessment. | |
| Juan Pablo Burgue et al. [28] | Drug susceptibility test (doxorubicin; ciprofloxacin; epirubicin; mitomycin C; thiotepa) | 40 cases | Each well was cultured with three mature organoids and treated with 0.2 mg/mL ciprofloxacin for 3 days. Different concentrated epirubicin, thiotepa, mitomycin C, and ciprofloxacin were added. After 2 hours of incubation, single-cell suspensions were obtained by treatment with 0.25% EDTA, and cell viability in each well was finally calculated using a trypan blue exclusion assay. |
| Jasper Mullenders et al. [32] | Drug susceptibility test (epirubicin; mitomycin C; gemcitabine; vincristine; doxorubicin; cisplatin) | 53 cases | The organoids were split with TrypLE, filtered through a 70-µm filter, re-cultured in BME, and counted after two days. Each well of ٣٨٤-well plates was placed with ١,٠٠٠ organoids in a medium containing ٥٪ BME. The drugs with indicated concentrations (٠.٠١‒١٠ μM gradient) were then added into the well, followed by culturing for 5 days. Cell viability was measured using the CellTiter-Glo 3D. |
| Robson Amaral et al. [33] | Drug susceptibility test (cisplatin, gemcitabine) | Each well of 96-well plates was placed with 1,000 tumor spheroids and treated with 10 μM drugs (cisplatin, Gemcitabine) for 24, 48, and 72 hours. The cell viability was finally assessed with CellTiter Glo 3D. |
Identifying the biochemical elements present in the microenvironment of cultured cells is crucial because the microenvironment of cells strongly influences behavior and function of cells [35]. It is also necessary to ensure the fluid dynamics in 3D cell culture since in vivo cells reside in a dynamic microenvironment [36]. The biophysical characteristics of hydrogels and real tissues are quite similar since both have strong water retention capabilities [37]. The dynamic process of cells is ensured by hydrogels, which act as an effective 3D culture matrix. By adjusting the parameters in the hydrogel manufacturing process, such as the macromolecular concentration, cross-linking degree, cross-linking conditions, pore size, cell loading efficiency, and swelling ratio in the culture environment, the biophysical properties of hydrogels, such as stiffness, degradation time, and biocompatibility, can be well-designed and controlled, hence controlling the cell behaviors [38]. In organoid culture, in addition to the Matrigel matrix as the main hydrogel, other supplements are listed in Table 3 [30,32,39-44]. In summary, determining medium composition and hydrogel parameters is critical in 3D cell culturing.
Table 3 Bladder cancer cell culture
| Cell | Culture medium | Supplements | Verification method | References |
|---|---|---|---|---|
| Human cells | Advanced DMEM/F12; | GlutaMAX; B27; EGF; human FGF-basic | The urothelial cells were isolated from the human urinary tract by enzymatic digestion and selected with flow cytometry. The isolated cells were then infected with lentivirus containing five genetic factors and cultured in organoid culture. IF staining was used for comparison. | 39 |
| Human Cells | Advanced DMEM/F-12; | GlutaMAX; HEPES, B27; N-Acetyl-L-cysteine; nicotinamide; A83-01; R-spondin-1; Noggin; EGF; FGF2/10; SB202190 | Hematoxylin and eosin (H&E) staining was used to demonstrate similar tissue morphology to the epithelial component of the original tumor tissues by histological examination. Immunofluorescence analysis and RNA-seq were performed, and the results showed that the marker expression was consistent between tumor tissue and its derived organoids. | 40 |
| Mouse cells | Advanced DMEM/F12; | HEPES; Nicotinamide; N-acetyl-L-cysteine; GlutaMAX; penicillin/streptomycin; mouse EGF; B-27; A8301; Y-27632 | bladder tumor organoids derived from BBN-induced urothelial carcinoma were cultured in vitro and treated with 5’-azacitidine. Organoid functions were verified through analyzing the degree of methylation induced by 5’-azacitidine using bisulfite sequencing. | 41 |
| Mouse Cells | DMEM/Ham’s F12 | Hydrocortisone; EGF; penicillin; streptomycin; amphotericin B (PAA). | Four different urothelial cell isolation methods were compared by analyzing protein expression of markers CK7, 8, 18 and p63 stained by IHC and IF. | 42 |
| Human cells and mouse cells | Advanced DMEM/F12; | Murine primary cells: Adv DMEM/F-12; FGF10; FGF7; A83-01 (500 nM); B27; Y-27632; Human primary cells: Adv DMEM/F-12; FGF10; FGF7; FGF2; B27; A83-01; N-acetylcysteine; nicotinamide; Y-27632; | Ditto | 32 |
| Human Cells | Waymouth’s MB 752/1 | 10% FBS; hydrocortisone hemisuccinate (Sigma-Aldrich); ferrous sulphate; vitamin C; | The organoids were produced by culturing normal human urothelial cells with appropriate substrates. The urothelial differentiation-related markers E-cadherin, β1-integrin, and CD44 expression were immunohistologically analyzed. | 44 |
| Human Cells | hepatocyte culture medium | EGF; FBS; Y-27632; GlutaMAX; primocin | The indicated markers were stained with H&E and IF, and the organoid was compared to the genes of primary cancer tissues using RNA-seq for consistency. | 30 |
| Dog-derived cells | advanced DMEM/F-12; | Wnt; Noggin; R-spondin-; GlutaMAX; Primocin; N-Acetyl-L-cysteine; nicotinamide; mouse EGF; A83-01 | The BC organoids were generated from urine samples of dogs with BC and were subjected to WB, HE, and Prestoblue cell viability assays. | 43 |
3.2 3D tissue models by bioprinting
3D bioprinting uses cells, extracellular matrix, biological factors, and biomaterials as raw materials to manufacture biological tissues as living products [45]. 3D bioprinting employs different strategies of bio-ink deposition, depending on the specific type of technique being used. Cells and biomaterials are deposited to build structures mimicking tissues or organs, which can serve as tools for development of personalized medicines and tissue engineering [46]. In 1981, Dr. Hideo Kodama, for the first time, proposed the concept of 3D bioprinting, and then Charles Chuck Hull released the first 3D biological printer in 1993, which ushered in a new era of 3D bioprinting technology [47].
Basic steps of 3D bioprinting include: (1) designing construct structures with the aid of 3D computational modeling; (2) The complex bio-ink includes biomaterials and cells, which are bio-printed to form tissues; (3) coordinating multicellular tissues to achieve the expected/desired physiological or pathological functions. Nowadays, 3D bioprinting techniques can be divided into three major types: inkjet-based 3D bioprinting, extrusion-based 3D bioprinting, and light-based 3D bioprinting, such as digital-light processing (DLP). Table 4 compares the pros and cons of the three bioprinting technologies [48-52].
Table 4 Comparison of three 3D bioprinting technologies
| Inkjet | Extrusion | Light | References | |
|---|---|---|---|---|
| Cell density | <106 cells/mL | <108 cells/mL | <108 cells/mL | 48 |
| Print speed | Fast | low | Medium | 52 |
| Resolution | High | Moderate | High | 49 |
| Bio-ink | Alginate, PEGDMA, Collagen | Alginate, GelMA, Collagen | GelMA, Hyaluronic acid, Alginate, Silk fibroin | 50,51 |
With the continuous improvement of 3D bioprinting technology, researchers have resolved many bottleneck problems encountered, such as tissue manufacturing with immune responses, complex neural networks, personalized metabolic models, and stepped into new frontiers, such as high-throughput drug screening.
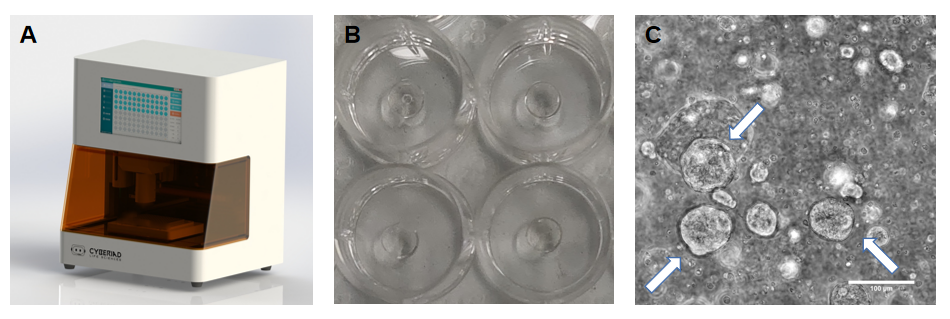
Dr. Tanan Bejrananda, after radical cystectomy, successfully transplanted a 3D-bioprinted extracorporeal y-bag new bladder into a 48-year-old MIBC patient. The operation improves the postoperative quality of life of patients and provides a new treatment for managing BC [53]. In addition, Atala et al. [48] cultured urothelial cells and muscle cells from 7 patients with bladder cancer and inoculated them onto biodegradable bladder-shaped scaffolds formed by 3D bioprinting of collagen or collagen/polyglycolic acid composites. A series of urodynamic, cystographical, ultrasonographic studies, bladder biopsy, and blood cell analysis showed that the average bladder leakage point pressure was reduced, while the volume and the compliance of the composite engineered bladder with omentum-wrapping increased, and the intestinal function recovered rapidly after the operation. Myeong Joo Kim et al. [54] used gelatin methacryloyl (GelMA) to 3D-print 5637 cell scaffolds. The cell proliferation efficiency of 5637 and T24 was significantly higher than that of 2D cultured cells, and the secretion of E-cadherin, an intercellular interaction protein in the 5637 cells, was higher. The evaluation of antibiotics rapamycin, BCG, and other anticancer drugs using the 3D bioprinted model showed that 5637 cells had higher drug resistance and lower sensitivity in 3D culture. Furthermore, DLP 3D bioprinting allowed for the establishment of highly reproducible patient-derived tissues (PDT) by cultivating cells isolated from patients' bladder cancer specimens on a biomimetic hydrogel matrix. The bioprinted bladder PDT can preserve primary cells for weeks and pave the way to the future personalized therapy (Fig.1). The findings support that 3D bioprinting technology can simulate the microenvironment of human bladder cancer and help achieve efficient drug screening. Bladder cancer patients may receive a customized course of treatment with increased safety and lower costs.
Figure 1 A. The DLP Bioprinter (DLP Bioprinter R1, Cyberiad Intelligent Technology) used for generating reproducible bladder cancer PDTs. B. Photo of 3D bioprinted, hydrogel-based, primary patient cell-encapsulating PDTs in well plates. C. Bright field images of bladder cancer PDT in 3D bioprinted constructs after 3 days of culture.
White arrow: organoids-like structures formed within PDT. Scale bar =100 μm.
White arrow: organoids-like structures formed within PDT. Scale bar =100 μm.
3.3 Microfluidic 3D tissue models
Microfluidic devices, also known as lab-on-a-chip, integrate the basic operating units of sample preparation, reaction, separation, and detection in biological, chemical, and medical analyses into a micro-scale chip to automatically complete the whole process of experimental analysis. Microfluidic chips-based 3D tissue models are potent tools for simulating in vitro physiologically-relevant microenvironments, since 3D cell culture in microfluidic chips can 3-dimentionally reproduce the dynamics of native tissues that conventional 3D culture methods cannot replicate.
Microfluidic models overcome many difficulties associated with 3D sphere culture and organoid growing in Matrigel or other hydrogels, and can induce the cell diversity in a complete tissue structure and test single-cell drug sensitivity [55]. Kim et al. [56] developed a microfluidic chip for bladder cancer. T24, MRC-5, HUVEC, and THP-1 were co-cultured in the microfluidic chip. The results showed that the cell viability was the best under the condition of 15% filling density of the circular chamber and 20 μL/min microflow velocity. Meanwhile, the immune response of the 3D tissue cultured in the microfluidic chip increased with the concentration of the anticancer drug BCG.
Even though the organ-on-a-chip model is expected to help screen anticancer drugs, some challenges remain. For example, working out appropriate experimental methods for evaluating the microenvironment of multicellular co-culture and the high-throughput fabrication of chips is challenging. This means that further technological development is required before this technique can be applied more widely in the study of bladder cancer.
We created a table (Table 5) that compares the differences among the three 3D culture methods.
Table 5 Comparison of three 3D cultures
| Organoids | 3D tissue models by bioprinting | Microfluidic 3D tissue models | |
|---|---|---|---|
| Preparation cycle | middle | fast | fast |
| Modeling success rate | middle | high | High, high technical requirements |
| Physiological, clinically relevant | Semi-physiological | Semi-physiological | Semi-physiological |
| Genetic information fidelity | high | high | high |
| Model reproducibility and controllability | middle | high | high |
| Human-derived cell-cell interactions | Tumor cells predominate | Contains different cells | Contains different cells |
| Matrix material controllability | limited | Clear matrix composition | Clear matrix composition |
| cost | middle | high | high |
| flux | middle | high | high |
4. Conclusion
Bladder cancer is a malignancy which is pathophysiologically multifactorial and complicated. To provide a more secure and efficient technique for treating bladder cancer, it is vital for researchers to understand the molecular processes underlying the development and progression of bladder cancer.
Animal models and 2D cell models are now the main research tools used to study the molecular mechanism of bladder cancer, both having reached a relatively advanced stage. The limitations of these conventional models, however, prevent their further application in bladder cancer research. Protracted time cycles, high costs, and a lower success rate are some of the drawbacks of animal models. Additionally, creating intricate animal models requires specialized expertise, but due to species variations, they still fall short of accurately simulating the biological behavior of human bladder cancer. Due to differences in genetic traits, 2D cell culture cannot perfectly replicate the state of cells in vivo.
In order to replicate the dynamic microenvironment of cells in vivo, the field is evolving towards 3D cell culture technology, which will tremendously push forward bioengineering and the pharmaceutical researches. 3D cultured cells can better mimic physiologically-relevant behavior of bladder tumor cells and the drug-elicited mechanotransduction. State-of-the-art 3D culture models include organoid, 3D-bioprinted, and microfluidic tissue models. Organoid models and 3D bioprinting have been growing rapidly and demonstrating great potential for broad applications, and microfluidics is still a relatively niche field for bladder cancer research. The most promising technology among all the revolutionary 3D cell culture methods is likely the 3D bioprinting since it offers researchers flexibility on cell composition, material composition, and spatial organization of cellular and biomaterials within the bioprinted tissue constructs to best mimic the native tissue microenvironments. The more biomimetic 3D models can potentially accelerate drug development and minimize our reliance on animal testing.
Acknowledgments
The authors are indebted to Professor Gongxian Wang for his guidance.
References
- Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol. 2017 Jan;71(1):96–108. https://doi.org/10.1016/j.eururo.2016.06.010 PMID: 27370177
- Chen W, Xia C, Zheng R, Zhou M, Lin C, Zeng H, et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: a comparative risk assessment. Lancet Glob Health. 2019 Feb;7(2):e257–69. https://doi.org/10.1016/S2214-109X(18)30488-1 PMID: 30683243
- Puzio-Kuter AM, Castillo-Martin M, Kinkade CW, Wang X, Shen TH, Matos T, et al. Inactivation of p53 and Pten promotes invasive bladder cancer. Genes Dev. 2009 Mar;23(6):675–80. https://doi.org/10.1101/gad.1772909 PMID: 19261747
- Langhans SA. Three-Dimensional in Vitro Cell Culture Models in Drug Discovery and Drug Repositioning. Front Pharmacol. 2018 Jan;9:6. https://doi.org/10.3389/fphar.2018.00006 PMID: 29410625
- Ravi M, Paramesh V, Kaviya SR, Anuradha E, Solomon FD. 3D cell culture systems: advantages and applications. J Cell Physiol. 2015 Jan;230(1):16–26. https://doi.org/10.1002/jcp.24683 PMID: 24912145
- Imamura Y, Mukohara T, Shimono Y, Funakoshi Y, Chayahara N, Toyoda M, et al. Comparison of 2D- and 3D-culture models as drug-testing platforms in breast cancer. Oncol Rep. 2015 Apr;33(4):1837–43. https://doi.org/10.3892/or.2015.3767 PMID: 25634491
- Bodgi L, Bahmad HF, Araji T, Al Choboq J, Bou-Gharios J, Cheaito K, et al. Assessing Radiosensitivity of Bladder Cancer in vitro: A 2D vs. 3D Approach. Front Oncol. 2019 Mar;9:153. https://doi.org/10.3389/fonc.2019.00153 PMID: 30941305
- Ikari R, Mukaisho KI, Kageyama S, Nagasawa M, Kubota S, Nakayama T, et al. Differences in the Central Energy Metabolism of Cancer Cells between Conventional 2D and Novel 3D Culture Systems. Int J Mol Sci. 2021 Feb;22(4):1805. https://doi.org/10.3390/ijms22041805 PMID: 33670390
- Jiang X, Lei T, Zhang M. Expression and Functions of Formyl Peptide Receptor 1 in Drug-Resistant Bladder Cancer. Technol Cancer Res Treat. 2018 Jan;17:1533034618769413. https://doi.org/10.1177/1533034618769413 PMID: 29665744
- Yu S, Meng Q, Hu H, Zhang M. Correlation of ANXA1 expression with drug resistance and relapse in bladder cancer. Int J Clin Exp Pathol. 2014 Aug;7(9):5538–48. PMID: 25337195
- Zuiverloon TC, de Jong FC, Costello JC, Theodorescu D. Systematic Review: Characteristics and Preclinical Uses of Bladder Cancer Cell Lines. Bladder Cancer. 2018 Apr;4(2):169–83. https://doi.org/10.3233/BLC-180167 PMID: 29732388
- Jamieson LE, Harrison DJ, Campbell CJ. Chemical analysis of multicellular tumour spheroids. Analyst (Lond). 2015 Jun;140(12):3910–20. https://doi.org/10.1039/C5AN00524H PMID: 25923379
- Reis LO, Pereira TC, Favaro WJ, Cagnon VH, Lopes-Cendes I, Ferreira U. Experimental animal model and RNA interference: a promising association for bladder cancer research. World J Urol. 2009 Jun;27(3):353–61. https://doi.org/10.1007/s00345-009-0374-4 PMID: 19214530
- Oliveira PA, Arantes-Rodrigues R, Vasconcelos-Nóbrega C. Animal models of urinary bladder cancer and their application to novel drug discovery. Expert Opin Drug Discov. 2014 May;9(5):485–503. https://doi.org/10.1517/17460441.2014.902930 PMID: 24670247
- Asanuma H, Arai T, Seguchi K, Kawauchi S, Satoh H, Kikuchi M, et al. Successful diagnosis of orthotopic rat superficial bladder tumor model by ultrathin cystoscopy. J Urol. 2003 Feb;169(2):718–20. https://doi.org/10.1016/S0022-5347(05)64000-1 PMID: 12544350
- Holmäng S, Cano M, Grenabo L, Hedelin H, Johansson SL. Effect of indomethacin on N-[4-(5-nitro-2-furyl)-2-thiazolyl]formamide-induced urinary tract carcinogenesis. Carcinogenesis. 1995 Jul;16(7):1493–8. https://doi.org/10.1093/carcin/16.7.1493 PMID: 7614682
- Montie JE. Profiling the evolution of human metastatic bladder cancer. J Urol. 2005 Aug;174(2):485–6. https://doi.org/10.1097/01.ju.0000171071.88466.cc PMID: 16006872
- Watanabe T, Shinohara N, Sazawa A, Harabayashi T, Ogiso Y, Koyanagi T, et al. An improved intravesical model using human bladder cancer cell lines to optimize gene and other therapies. Cancer Gene Ther. 2000 Dec;7(12):1575–80. https://doi.org/10.1038/sj.cgt.7700261 PMID: 11228536
- Wilmanns C, Fan D, Obrian C, Radinsky R, Bucana C, Tsan R, et al. Modulation of Doxorubicin sensitivity and level of p-glycoprotein expression in human colon-carcinoma cells by ectopic and orthotopic environments in nude-mice. Int J Oncol. 1993 Sep;3(3):413–22. https://doi.org/10.3892/ijo.3.3.413 PMID: 21573380
- Overdevest JB, Thomas S, Kristiansen G, Hansel DE, Smith SC, Theodorescu D. CD24 offers a therapeutic target for control of bladder cancer metastasis based on a requirement for lung colonization. Cancer Res. 2011 Jun;71(11):3802–11. https://doi.org/10.1158/0008-5472.CAN-11-0519 PMID: 21482678
- Costa EC, Moreira AF, de Melo-Diogo D, Gaspar VM, Carvalho MP, Correia IJ. 3D tumor spheroids: an overview on the tools and techniques used for their analysis. Biotechnol Adv. 2016 Dec;34(8):1427–41. https://doi.org/10.1016/j.biotechadv.2016.11.002 PMID: 27845258
- Patel VG, Oh WK, Galsky MD. Treatment of muscle-invasive and advanced bladder cancer in 2020. CA Cancer J Clin. 2020 Sep;70(5):404–23. https://doi.org/10.3322/caac.21631 PMID: 32767764
- Zhang ZT, Pak J, Shapiro E, Sun TT, Wu XR. Urothelium-specific expression of an oncogene in transgenic mice induced the formation of carcinoma in situ and invasive transitional cell carcinoma. Cancer Res. 1999 Jul;59(14):3512–7. PMID: 10416618
- Kompier LC, Lurkin I, van der Aa MN, van Rhijn BW, van der Kwast TH, Zwarthoff EC. FGFR3, HRAS, KRAS, NRAS and PIK3CA mutations in bladder cancer and their potential as biomarkers for surveillance and therapy. PLoS One. 2010 Nov;5(11):e13821. https://doi.org/10.1371/journal.pone.0013821 PMID: 21072204
- Ayala de la Peña F, Kanasaki K, Kanasaki M, Tangirala N, Maeda G, Kalluri R. Loss of p53 and acquisition of angiogenic microRNA profile are insufficient to facilitate progression of bladder urothelial carcinoma in situ to invasive carcinoma. J Biol Chem. 2011 Jun;286(23):20778–87. https://doi.org/10.1074/jbc.M110.198069 PMID: 21388952
- Badr-Eldin SM, Aldawsari HM, Kotta S, Deb PK, Venugopala KN. Three-Dimensional In Vitro Cell Culture Models for Efficient Drug Discovery: Progress So Far and Future Prospects. Pharmaceuticals (Basel). 2022 Jul;15(8):926. https://doi.org/10.3390/ph15080926 PMID: 36015074
- Knight E, Przyborski S. Advances in 3D cell culture technologies enabling tissue-like structures to be created in vitro. J Anat. 2015 Dec;227(6):746–56. https://doi.org/10.1111/joa.12257 PMID: 25411113
- Burgués JP, Gómez L, Pontones JL, Vera CD, Jiménez-Cruz JF, Ozonas M. A chemosensitivity test for superficial bladder cancer based on three-dimensional culture of tumour spheroids. Eur Urol. 2007 Apr;51(4):962–9. https://doi.org/10.1016/j.eururo.2006.10.034 PMID: 17084017
- Medle B, Sjödahl G, Eriksson P, Liedberg F, Höglund M, Bernardo C. Patient-Derived Bladder Cancer Organoid Models in Tumor Biology and Drug Testing: A Systematic Review. Cancers (Basel). 2022 Apr;14(9):2062. https://doi.org/10.3390/cancers14092062 PMID: 35565191
- Lee SH, Hu W, Matulay JT, Silva MV, Owczarek TB, Kim K, et al. Tumor Evolution and Drug Response in Patient-Derived Organoid Models of Bladder Cancer. Cell. 2018 Apr;173(2):515–528.e17. https://doi.org/10.1016/j.cell.2018.03.017 PMID: 29625057
- Elbadawy M, Usui T, Mori T, Tsunedomi R, Hazama S, Nabeta R, et al. Establishment of a novel experimental model for muscle-invasive bladder cancer using a dog bladder cancer organoid culture. Cancer Sci. 2019 Sep;110(9):2806–21. https://doi.org/10.1111/cas.14118 PMID: 31254429
- Mullenders J, de Jongh E, Brousali A, Roosen M, Blom JP, Begthel H, et al. Mouse and human urothelial cancer organoids: A tool for bladder cancer research. Proc Natl Acad Sci USA. 2019 Mar;116(10):4567–74. https://doi.org/10.1073/pnas.1803595116 PMID: 30787188
- Amaral R, Zimmermann M, Ma AH, Zhang H, Swiech K, Pan CX. A Simple Three-Dimensional In Vitro Culture Mimicking the In Vivo-Like Cell Behavior of Bladder Patient-Derived Xenograft Models. Cancers (Basel). 2020 May;12(5):1304. https://doi.org/10.3390/cancers12051304 PMID: 32455634
- Lamy P, Nordentoft I, Birkenkamp-Demtröder K, Thomsen MB, Villesen P, Vang S, et al. Paired Exome Analysis Reveals Clonal Evolution and Potential Therapeutic Targets in Urothelial Carcinoma. Cancer Res. 2016 Oct;76(19):5894–906. https://doi.org/10.1158/0008-5472.CAN-16-0436 PMID: 27488526
- Breslin S, O’Driscoll L. Three-dimensional cell culture: the missing link in drug discovery. Drug Discov Today. 2013 Mar;18(5-6):240–9. https://doi.org/10.1016/j.drudis.2012.10.003 PMID: 23073387
- Buchanan CF, Verbridge SS, Vlachos PP, Rylander MN. Flow shear stress regulates endothelial barrier function and expression of angiogenic factors in a 3D microfluidic tumor vascular model. Cell Adhes Migr. 2014;8(5):517–24. https://doi.org/10.4161/19336918.2014.970001 PMID: 25482628
- Sackett SD, Tremmel DM, Ma F, Feeney AK, Maguire RM, Brown ME, et al. Extracellular matrix scaffold and hydrogel derived from decellularized and delipidized human pancreas. Sci Rep. 2018 Jul;8(1):10452. https://doi.org/10.1038/s41598-018-28857-1 PMID: 29993013
- Odawara A, Gotoh M, Suzuki I. Control of neural network patterning using collagen gel photothermal etching. Lab Chip. 2013 Jun;13(11):2040–6. https://doi.org/10.1039/c3lc00036b PMID: 23615759
- Wang L, Smith BA, Balanis NG, Tsai BL, Nguyen K, Cheng MW, et al. A genetically defined disease model reveals that urothelial cells can initiate divergent bladder cancer phenotypes. Proc Natl Acad Sci USA. 2020 Jan;117(1):563–72. https://doi.org/10.1073/pnas.1915770117 PMID: 31871155
- Yu L, Li Z, Mei H, Li W, Chen D, Liu L, et al. Patient-derived organoids of bladder cancer recapitulate antigen expression profiles and serve as a personal evaluation model for CAR-T cells in vitro. Clin Transl Immunology. 2021 Jan;10(2):e1248. https://doi.org/10.1002/cti2.1248 PMID: 33552510
- Kim S, Kim Y, Kong J, Kim E, Choi JH, Yuk HD, et al. Epigenetic regulation of mammalian Hedgehog signaling to the stroma determines the molecular subtype of bladder cancer. eLife. 2019 Apr;8:e43024. https://doi.org/10.7554/eLife.43024 PMID: 31036156
- Kloskowski T, Uzarska M, Gurtowska N, Olkowska J, Joachimiak R, Bajek A, et al. How to isolate urothelial cells? Comparison of four different methods and literature review. Hum Cell. 2014 Apr;27(2):85–93. https://doi.org/10.1007/s13577-013-0070-y PMID: 24368576
- Ringuette Goulet C, Bernard G, Chabaud S, Couture A, Langlois A, Neveu B, et al. Tissue-engineered human 3D model of bladder cancer for invasion study and drug discovery. Biomaterials. 2017 Nov;145:233–41. https://doi.org/10.1016/j.biomaterials.2017.08.041 PMID: 28888113
- Varley CL, Southgate J. Organotypic and 3D reconstructed cultures of the human bladder and urinary tract. Methods Mol Biol. 2011;695:197–211. https://doi.org/10.1007/978-1-60761-984-0_13 PMID: 21042974
- Gu Q, Hao J, Lu Y, Wang L, Wallace GG, Zhou Q. Three-dimensional bio-printing. Sci China Life Sci. 2015 May;58(5):411–9. https://doi.org/10.1007/s11427-015-4850-3 PMID: 25921944
- Hansen CJ, Saksena R, Kolesky DB, Vericella JJ, Kranz SJ, Muldowney GP, et al. High-throughput printing via microvascular multinozzle arrays. Adv Mater. 2013 Jan;25(1):96–102. https://doi.org/10.1002/adma.201203321 PMID: 23109104
- Abdella S, Youssef SH, Afinjuomo F, Song Y, Fouladian P, Upton R, et al. 3D Printing of Thermo-Sensitive Drugs. Pharmaceutics. 2021 Sep;13(9):1524. https://doi.org/10.3390/pharmaceutics13091524 PMID: 34575600
- Murphy SV, Atala A. 3D bioprinting of tissues and organs. Nat Biotechnol. 2014 Aug;32(8):773–85. https://doi.org/10.1038/nbt.2958 PMID: 25093879
- Ozbolat IT, Yu Y. Bioprinting toward organ fabrication: challenges and future trends. IEEE Trans Biomed Eng. 2013 Mar;60(3):691–9. https://doi.org/10.1109/TBME.2013.2243912 PMID: 23372076
- Wang Z, Abdulla R, Parker B, Samanipour R, Ghosh S, Kim K. A simple and high-resolution stereolithography-based 3D bioprinting system using visible light crosslinkable bioinks. Biofabrication. 2015 Dec;7(4):045009. https://doi.org/10.1088/1758-5090/7/4/045009 PMID: 26696527
- Nahmias Y, Schwartz RE, Verfaillie CM, Odde DJ. Laser-guided direct writing for three-dimensional tissue engineering. Biotechnol Bioeng. 2005 Oct;92(2):129–36. https://doi.org/10.1002/bit.20585 PMID: 16025535
- Guillotin B, Souquet A, Catros S, Duocastella M, Pippenger B, Bellance S, et al. Laser assisted bioprinting of engineered tissue with high cell density and microscale organization. Biomaterials. 2010 Oct;31(28):7250–6. https://doi.org/10.1016/j.biomaterials.2010.05.055 PMID: 20580082
- Bejrananda T, Liawrungrueang W. Successful transitional cell carcinoma of bladder underwent laparoscopic radical cystectomy with orthotopic intracorporeal Y pouch neobladder using a 3D digital printing model for surgical post op pouch evaluation. Urol Case Rep. 2020 Apr;31:101190. https://doi.org/10.1016/j.eucr.2020.101190 PMID: 32292705
- Kim MJ, Chi BH, Yoo JJ, Ju YM, Whang YM, Chang IH. Structure establishment of three-dimensional (3D) cell culture printing model for bladder cancer. PLoS One. 2019 Oct;14(10):e0223689. https://doi.org/10.1371/journal.pone.0223689 PMID: 31639124
- Sontheimer-Phelps A, Hassell BA, Ingber DE. Modelling cancer in microfluidic human organs-on-chips. Nat Rev Cancer. 2019 Feb;19(2):65–81. https://doi.org/10.1038/s41568-018-0104-6 PMID: 30647431
- Kim JH, Lee S, Kang SJ, Choi YW, Choi SY, Park JY, et al. Establishment of Three-Dimensional Bioprinted Bladder Cancer-on-a-Chip with a Microfluidic System Using Bacillus Calmette-Guérin. Int J Mol Sci. 2021 Aug;22(16):8887. https://doi.org/10.3390/ijms22168887 PMID: 34445591