
Download

Bladder | 2023 | Vol. 10 | e21200013
DOI: 10.14440/bladder.2023.872
DOI: 10.14440/bladder.2023.872
ARTICLE
Patterns of chemotherapy use in muscle-invasive bladder cancer in a tertiary centre
Kylie Yen-Yi Lim1,2, Kevin Chu1, Nieroshan Rajarubendra1, James Huang1, David Pook3, Paul Manohar1, Matthew Harper1, Scott Donnellan1, Weranja Ranasinghe1,4
1Department of Urology, Monash Health, Casey, VIC, Australia
2School of Clinical Sciences, Monash University, Clayton, VIC, Australia
3Department of Oncology, Monash Health, Clayton, VIC, Australia
4Department of Anatomy and Developmental Biology, Monash University, Clayton, VIC, Australia
2School of Clinical Sciences, Monash University, Clayton, VIC, Australia
3Department of Oncology, Monash Health, Clayton, VIC, Australia
4Department of Anatomy and Developmental Biology, Monash University, Clayton, VIC, Australia
*Corresponding author: Dr Kylie Yen-Yi Lim, Department of Urology, Monash Health – Casey Hospital , 62-70 Kangan Dr, Berwick, Victoria 3806; Phone +61 9594 6666; Email: kylielim7@gmail.com; https://orcid.org/0000-0003-3370-3530
Declaration of interests: There is no conflict of interest associated with this publication and no financial support was required at time of submission.
Abbreviation used: AC, adjuvant chemotherapy; CTCAE, common terminology criteria for adverse events; CTCAP, computerised tomography chest, abdominal and pelvic; ddMVAC, dose dense methotrexate vinblastine doxorubicin cisplatin; IQR, interquartile range; MIBC, muscle invasive bladder cancer; NAC, neoadjuvant chemotherapy; NCDB, National Cancer Database; NYHA, New York Heart Association; RECIST, response evaluation criteria in solid tumours; RC, radical cystectomy; SEER, Surveillance, Epidemiology and End Results; TURBT, transurethral resection of bladder tumour
Received October 13, 2023; Revision received November 27, 2023; Accepted November 28, 2023; Published December 11,2023
Abstract
Objectives: Although neoadjuvant chemotherapy (NAC) has been demonstrated to have significant benefits to survival in patients with muscle-invasive bladder cancer (MIBC), the current utilization of NAC in Australia is unknown. The aim of this study was to evaluate the patterns of neoadjuvant and adjuvant chemotherapy (AC) use in patients undergoing cystectomy for MIBC at a large tertiary institution in Australia.
Methods: A retrospective study was conducted using data of patients who underwent a radical cystectomy (RC) at a high-volume centre for MIBC between 2011 and 2021.
Results: Of 69 patients who had a cystectomy for ≥ pT2 bladder cancer, 73.9% were eligible for NAC. However, of those eligible, only five patients received NAC (9.8%). Of the total patients who were eligible for AC, only 44.4% received postoperative chemotherapy. Common reasons for the lack of uptake were due to patients being unfit or declining treatment. There was no difference in progression-free survival or overall survival in those who received NAC and AC.
Conclusions: The majority of patients undergoing RC for MIBC received AC compared to NAC, reflecting the real-world challenge of NAC uptake. This highlights the need for ongoing improvements in selection and usage of NAC and less reliance of AC utilization post RC.
Keywords: Adjuvant chemotherapy, chemotherapy, cystectomy, neoadjuvant therapy, muscle-invasive bladder cancer
Introduction
Muscle-invasive bladder cancer (MIBC) is an aggressive disease with a propensity for rapid tumour progression, recurrence and metastasis. As such, the current evidence supports a 5% survival benefit with neoadjuvant chemotherapy (NAC) prior to radical cystectomy (RC) for MIBC [1]. Furthermore, NAC offers potential for down-staging of the primary tumour and can improve outcomes following surgery [2]. Guidelines from urological and oncological societies, including American Urological Association, European Association of Urology, the National Comprehensive Cancer Network and European Society for Medical Oncology, advocate for cisplatin-based NAC in MIBC [3-6]. Despite the survival benefits established with NAC, there has been evidence of slow uptake of NAC in studies internationally, owing to concerns regarding over-treatment and delay in time to surgery [7,8].
Adjuvant chemotherapy (AC) offers an alternative, as it can be given to patients with aggressive disease at RC, allowing for better candidate selection. Therefore, some clinicians advocate for AC, with a recent systematic review supporting cisplatin-based adjuvant therapy which resulted in an absolute survival improvement of 6% at 5 years [9]. However, the challenges of AC include delayed treatment of micro-metastatic disease and increased difficulty in administering chemotherapy due to postoperative morbidity [10]. With further developments in NAC, trends suggest there has been no increase in utilization of AC [11].
Real-world utilization and patterns of chemotherapy use in routine practice in Australia have been described in limited up-to-date studies [12]. Given the demonstrated benefits of perioperative chemotherapy, the aim of this study was to evaluate the patterns of NAC and AC use for MIBC at a large, tertiary centre in Australia.
Materials and Methods
Patients who underwent a radical cystectomy at a large tertiary institution in Victoria, Australia (MH) between 2011 and 2021 were retrospectively identified using Medicare benefits schedule codes. MH is the largest health service in Australia’s second most populous state, estimated to provide healthcare to one-quarter of the city’s population. Between 2020-2021, MH had more than 250,000 hospital admissions.
Patients who had a pathological diagnosis of ≥ pT2 and underwent an RC with curative intent were included. Demographic details, chemotherapy use and tumour data were collected from the institution’s medical records. Less than 5% of collated data was missing and were missing in categorical variables. The missing indicator method was applied.
All patients diagnosed with MIBC were discussed at the institution’s multidisciplinary meeting. Eligibility criteria for NAC were defined according to Galsky criteria [13]. This included WHO or ECOG performance status (PS) < 2 or Karnofsky PS of 60-70%, creatinine clearance (calculated or measured) ≥ 60 ml/min, Common Terminology Criteria for Adverse Events (CTCAE) v4 grade <2 audiometric hearing loss, CTCAE v4 grade <2 peripheral neuropathy, < New York Heart Association (NYHA) class III heart failure. Eligibility for AC was defined as patients with high-risk pathological features - pathological stage ≥T3a or lymph node involvement [14]. Response to chemotherapy was defined according to Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria [15]. The best overall response was defined during post-treatment assessment, prior to RC for NAC and most recent post-treatment assessment for AC.
All patients underwent computerized tomography chest, abdominal and pelvic (CTCAP) staging scans prior to RC. The surveillance protocol following RC depended on RC pathology. Low risk patients post RC were followed-up in clinic with staging CTCAP and serum blood tests. High risk patients were immediately referred to medical oncology for consultation. Chemotherapy agents, dosing and scheduling were selected as per individual patient evaluation by the medical oncology team. The most frequently used regimes of dose dense methotrexate vinblastine doxorubicin cisplatin (ddMVAC) and gemcitabine and cisplatin were generally scheduled for 4 cycles. Standard dosing followed according to an Australian consensus-driven treatment protocol (eviQ platform). Following AC, patients had restaging scans to assess response to chemotherapy (CTCAP or FDG-PET/CT), determined at the discretion of the treating physician.
Outcomes were examined using Mann-Whitney and Kaplan Meier survival analyses.
This study was approved by the local Human Research Ethics Committee (RES-21-0000-718Q - 81380).
Results
Of 115 patients that had a cystectomy, 69 received a radical cystectomy for ≥pT2 bladder cancer with curative intent. The median age was 68 years old. Fifty-four patients were men and 15 were women. Of the 69 patients, five (7.2%) patients received NAC prior to RC and 20 (29%) underwent AC. Nineteen (27.5%) patients developed metastases after RC. Nineteen (27.5%) died at a median follow-up of 15.6 months (interquartile range, IQR 4.7-37.7).
79.7% had urothelial carcinoma of the bladder at cystectomy pathology. Nine patients (13%) had variant histopathology on transurethral resection of bladder tumor (TURBT) and 19 on final cystectomy (27.5%). Nineteen patients had synchronous prostate cancer detected on radical cystoprostatectomy specimens.
Neoadjuvant chemotherapy
Fifty-one (73.9%) patients were eligible for NAC. Of the 18 patients ineligible for NAC, 13 (72.2%) had impaired creatinine clearance, three had audiometric hearing loss, three had an ECOG score of 2 and one patient had NYHA class III heart failure. A total of five (5/51, 9.8%) patients received NAC. NAC patient characteristics are detailed in Table 1. The median age of those who received NAC and those eligible but did not receive NAC were 69 and 67 respectively.
Three patients were treated with ddMVAC and two with gemcitabine and cisplatin.
In patients who underwent NAC, the median time from diagnosis to RC was 3.9 months (IQR 2.3-4.9) compared to 1.6 months (IQR 1.1-2.3) in patients who did not receive NAC (p = 0.025). However, median time from last cycle of NAC to RC was 1.3 months (IQR 1.2-1.8). Four (80%) had downstaging to pT1 disease at RC. One patient (20%) had upstaging of disease from pT2a at TURBT to pT3 at RC.
Adjuvant chemotherapy
Forty-five (65.2%) patients were eligible for AC. However, only 20 out of 45 (44.4%) eligible patients received AC. Of these 20 patients, three patients had N+ disease, eight had T3+N0 disease, and nine had T3+N+ disease. The median age of those who received AC was 64.5 compared to the median age of 70 of those who were eligible but did not receive AC.
The median time from cystectomy to first cycle of AC was 1.6 months (IQR 1.4-2.1).
Gemcitabine and cisplatin were most frequently used (55%) as AC followed by ddMVAC in 20% of the patients. The remaining documented patients received combination gemcitabine and carboplatin or FOLFOX (leucovorin calcium, fluorouracil and oxaliplatin). Five (25%) developed metastases. Six (30%) died following AC at a median time of 28.4 months from RC (IQR 9.5-42.9).
Table 1. Demographic details of patients who received NAC, AC and neither NAC nor AC
| Total N = 69 | Neoadjuvant chemotherapy treatment N = 5 | Adjuvant chemotherapy treatment N = 20 | No chemotherapy treatment N = 44 | |
|---|---|---|---|---|
| Gender, no. (%) | ||||
| Male | 54 (78.3) | 5 (100) | 17 (85) | 32 (72.7) |
| Female | 15 (21.7) | 0 | 3 (15) | 12 (27.3) |
| Age, no. (%) | ||||
| ≤50 | 7 (10.1) | 1 (20) | 4 (20) | 2 (4.5) |
| 51-60 | 8 (11.6) | 0 | 2 (10) | 6 (13.6) |
| 61-70 | 27 (39.1) | 2 (40) | 9 (45) | 16 (36.4) |
| 71-80 | 26 (37.7) | 2 (40) | 5 (25) | 19 (43.2) |
| >80 | 1 (1.5) | 0 | 0 | 1 (2.3) |
| Cisplatin eligibility, no. (%) | ||||
| ECOG < 2 | 66 (95.7) | 5 (100) | 18 (90) | 43 (97.7) |
| CrCl ≥ 60 ml/min | 56 (81.2) | 5 (100) | 15 (75) | 36 (81.8) |
| No audiometric hearing loss | 64 (92.8) | 4 (80) | 18 (90) | 42 (95.5) |
| No peripheral neuropathy | 69 (100) | 5 (100) | 20 (100) | 44 (100) |
| NYHA classification < III | 68 (98.6) | 5 (100) | 20 (100) | 43 (97.7) |
| High-risk stratification, no. (%) | ||||
| LVI present | 15 (21.7) | 2 (40) | 3 (15) | 10 (22.7) |
| Hydronephrosis | 27 (39.1) | 0 | 13 (65) | 14 (31.8) |
| Clinical stage prior to RC, no. (%) | ||||
| T2 | 56 (81.2) | 4 (80) | 14 (70) | 38 (86.3) |
| T2a | 10 (14.5) | 1 (20) | 5 (25) | 4 (9.1) |
| T3 | 2 (2.9) | 0 | 1 (5) | 1 (2.3) |
| T4 | 1 (1.4) | 0 | 0 | 1 (2.3) |
| Median time from TURBT to RC, months | 3.9 | 1.5 | 1.6 | |
| Downstaging of T disease (from TURBT to cystectomy histopath), no. (%) | 16 (23.2) | 4 (80) | 1 (5) | 11 (25) |
| Metastases post RC, no. (%) Median time to metastases (months) | 19 (27.5) 6.5 | 1 (20) 3.4 | 5 (25) 19.1 | 13 (29.5) 6.5 |
| Deaths, no. (%) Causes of death, no. Disease-related Surgical Other cancer Unknown | 18 (26.1) | 1 (20) 1 | 6 (30) 3 1 2 | 11 (0.25) 6 1 4 |
AC, adjuvant chemotherapy; CrCl, creatinine clearance; ECOG, Eastern Cooperative Oncology Group; LVI, lymphovascular invasion; TURBT, transurethral resection of bladder tumour; RC, radical cystectomy
Of the 25 patients who did not receive AC, 28% did not have the rationale documented, 20% were deemed unfit or the patient had declined treatment (Fig. 1). Three (12%) patients were classified as inappropriate for AC; one due to delays post RC, another patient due to avoiding immunosuppression in this high-risk patient during the COVID-19 pandemic and the third due to a rare variant histology.
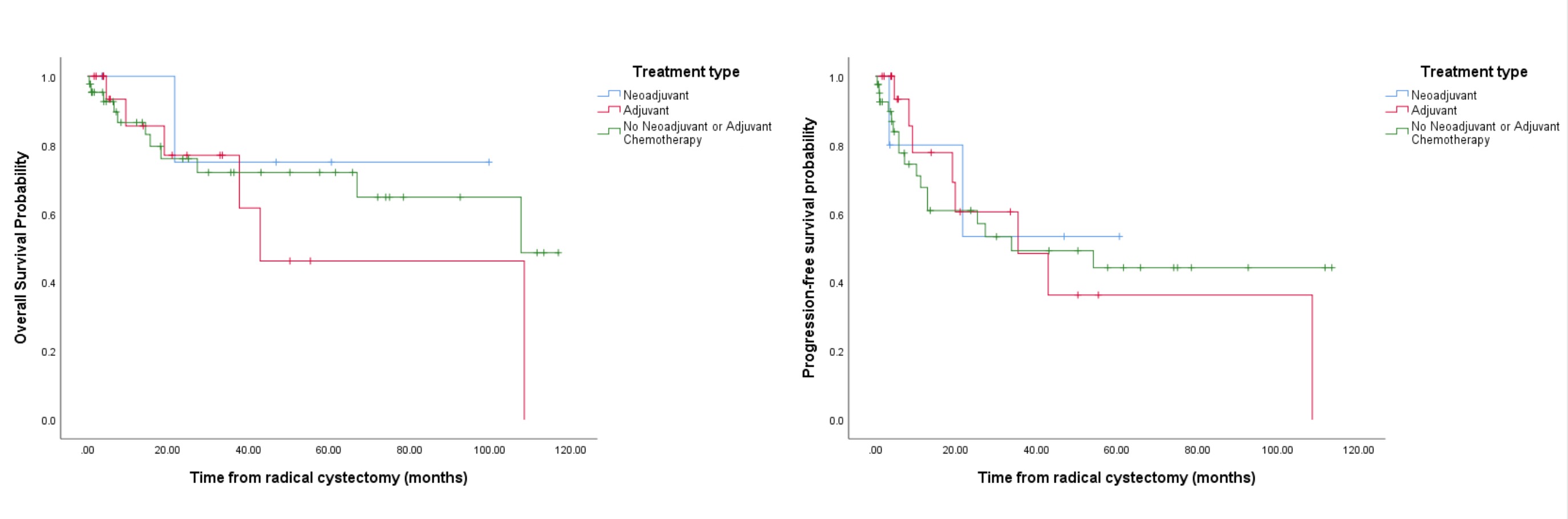
There was no difference in progression-free survival or overall survival between those who received NAC and AC (Fig. 2).
Figure 1. Reasons eligible patients did not receive adjuvant chemotherapy post radical cystectomy
Figure 2. Kaplan-Meier curves of overall survival probability and progression-free survival probability between patients who received NAC, AC and neither NAC nor AC. AC, adjuvant chemotherapy; NAC, neoadjuvant chemotherapy
There was also variation in treatment adjustments and response rates between patients who received NAC and AC (Table 2). Of the 20 patients who received AC, 25% of patients had progressive disease compared to 45% who had a complete clinical response.
Discussion
Our results demonstrated a low uptake of NAC, which was in keeping with some other local and international series. A previous Australian study reported NAC usage of 9.7%, equivalent to 9.8% at our institution [12]. Similarly, a large Canadian population study using the Ontario Cancer Registry identified NAC use of 4% [16]. United States National Cancer database (NCDB) between 1997 and 2003 also identified an 11.6% incidence of perioperative chemotherapy usage, with a low uptake of NAC representing 1.2% [17]. However, more recent US studies utilizing the NCDB and the Surveillance, Epidemiology and End Results (SEER) databases identified an increase in NAC usage of up to 32.3% in MIBC patients [11,18]. This growth has been attributed to the level-one evidence providing support for NAC use. There have also been developments to chemotherapy regimens to enhance the tolerability and minimize toxic effects that have made NAC a more appealing option. Despite this encouraging increase, a recent study from Yale, USA, involving 1,198 MIBC patients, reported that only 8% of patients received NAC [19]. The heterogeneity in NAC usage highlights the ongoing challenge of its uptake and variability seen regionally and globally based on factors such as high clinical cancer volumes, patient demographics, and clinician experience [8].
Table 2. Treatment adjustments and chemotherapy response in patients who received NAC and AC
| NAC | AC | |
|---|---|---|
| Treatment adjustments, no. (%) | ||
| Dose reduction | 1 (20) | 2 (10) |
| Early termination | 0 | 4 (20) |
| Full treatment received | 4 (80) | 9 (45) |
| Unknown | 0 | 5 (25) |
| Response, no. (%) | ||
| Clinical progressive disease | 0 | 5 (25) |
| Clinical stable disease | 3 (60) | 0 |
| Clinical partial response | 2 (40) | 0 |
| Clinical complete response | 0 | 9 (45) |
| Not evaluable | 0 | 6 (30) |
AC, adjuvant chemotherapy; NAC, neoadjuvant chemotherapy
In our study, four of the five (80%) patients who received NAC did not have progression of disease and had downstaging of clinical pathology at final RC. Despite this clinical advantage, 90.2% of eligible patients did not receive NAC. However, majority of decision points for patients proceeding straight to RC were not documented and are not known in this dataset. Multiple barriers have been identified in contributing to real-world NAC adherence. These include clinician factors such as lack of data awareness, bias and anecdotal experience; with patient factors including low health literacy, low socioeconomic status, and personal perceptions of chemotherapy and, in certain countries, insurance coverage along with patient compliance and access and institutional policies [8,20].
The main concerns for low NAC uptake relate to concerns surrounding surgical delay, over-treatment in organ-confined disease and progression in non-responders [10]. There was a delay of 10 weeks to RC in our study of those who received NAC compared to those who did not when comparing the time from TURBT to RC. However, our median time of 5.9 weeks (IQR 5.3-8) to RC following the last cycle of NAC was comparative to Beori et al who reported a median time to cystectomy following NAC of 7.6 weeks (IQR 5.2-10.8) in their cohort [21]. It has been suggested that patients can safely proceed to an RC 2.5-12 weeks after completing NAC without a difference in morbidity [22]. However, reducing delays can be facilitated through effective communication between the oncology and urology teams and other health professionals particularly during preparation for NAC.
While our results revealed one non-responder (20%) following NAC, only 30-40% of patients who received NAC experienced major responses on examination of RC pathology (defined as <ypT2 and ypN0) [23,24]. This highlights the difficulty of predicting patients’ response to NAC and importance of patient selection. Current clinical and pathological findings are not completely accurate predictors of NAC response. MD Anderson Cancer Centre has proposed additional risk stratification relying on features of hydronephrosis, clinical staging, aberrant pathology and lymphovascular invasion at TURBT to refine patient selection for NAC [25]. Although not yet available for routine practice, biomarkers like genomics and radiomics have shown initial promise in optimizing the precision of NAC responder identification [26].
One strategy used to overcome surgical delay and achieve appropriate patient selection for chemotherapy is the utilization of AC post RC, which was reflected by higher uptake of AC (44.4%) compared to NAC (9.8%) in eligible patients in our study. Choi et al demonstrated similar utilization trends of NAC and AC, at 6.4-12.2% and 23.4-21.3% respectively from 2004 to 2016 through analysis of a national Korean database [27]. Booth et al, in a Canadian population study, also demonstrated a higher utilization of AC compared to NAC (22% vs 4%) [16].
However, the utilization of AC depends on timely recovery post RC. Patients may develop complications like reduced renal function or performance status from RC which delays or precludes their eligibility to receive AC [28]. Compared to 20% in our cohort that was considered unfit post RC, a study at a high-volume tertiary centre found that 30% of 1,142 RC patients were unable to receive AC due to postoperative complications [10]. Thus, the reliance on AC alone should be carefully weighed against the benefits of NAC.
Furthermore, another concern about AC is the potential delay in the treatment of micro-metastatic disease, which may be present at time of diagnosis and is believed to be responsible for relapses [7]. 25% of our patients who received AC developed metastases. However, in a meta-analysis by Leow et al, cisplatin-based AC contributed to a 34% relative decrease in risk of disease recurrence compared to no AC [29]. Although this study provided greater confidence in AC, the evidence is not as robust due to flaws in several trials related to the study design and underpowered samples. Thus, the current standard of care for local MIBC remains as NAC followed by RC.
Our study was subject to several limitations, including those intrinsic to a retrospective study. Our study design may have missed patients with ≥ T2 disease who received ‘neoadjuvant’ chemotherapy and did not proceed to a cystectomy due to our inclusion criteria. Furthermore, long-term follow-up of some patients may not have been captured in our review as data depended on input from other centres. In addition, the small sample size of our study may not have adequate power to assess any benefits and survival outcomes.
Conclusion
Despite the improvements and benefits of perioperative chemotherapy, real-world adherence remains a challenge. The majority of patients undergoing RC for MIBC received AC, as compared to NAC at our institution. And while AC allows for better selection of candidates for chemotherapy post RC, a large proportion did not ultimately receive adjuvant therapy. Therefore, NAC should be considered in all patients undergoing RC. Further studies on biomarkers and other predictive tools may help identify NAC responders, which may result in broader acceptance of NAC. In the interim, ongoing multidisciplinary collaboration and clinician and patient education remain a vital component to improving and sustaining uptake of chemotherapy usage.
References
- Advanced Bladder Cancer Meta-analysis C. Neoadjuvant chemotherapy in invasive bladder cancer: a systematic review and meta-analysis. Lancet. 2003;361(9373):1927-34. Epub 2003/06/13. https://doi.org/10.1016/s0140-6736(03)13580-5. PMID: 12801735
- Eldefrawy A, Soloway MS, Katkoori D, Singal R, Pan D, Manoharan M. Neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer: The likelihood of initiation and completion. Indian J Urol. 2012;28(4):424-6. Epub 2013/03/02. https://doi.org/10.4103/0970-1591.105756. PMID: 23449818
- Chang SS, Bochner BH, Chou R, Dreicer R, Kamat AM, Lerner SP, et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J Urol. 2017;198(3):552-9. Epub 2017/05/01. https://doi.org/10.1016/j.juro.2017.04.086. PMID: 28456635
- Witjes JA, Bruins HM, Cathomas R, Comperat EM, Cowan NC, Gakis G, et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur Urol. 2021;79(1):82-104. Epub 2020/05/04. https://doi.org/10.1016/j.eururo.2020.03.055. PMID: 32360052
- Flaig TW, Spiess PE, Abern M, Agarwal N, Bangs R, Boorjian SA, et al. NCCN Guidelines(R) Insights: Bladder Cancer, Version 2.2022. J Natl Compr Canc Netw. 2022;20(8):866-78. Epub 2022/08/11. https://doi.org/10.6004/jnccn.2022.0041. PMID: 35948037
- Powles T, Bellmunt J, Comperat E, De Santis M, Huddart R, Loriot Y, et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(3):244-58. Epub 2021/12/04. https://doi.org/10.1016/j.annonc.2021.11.012. PMID: 34861372
- Raphael MJ, Booth CM. Neoadjuvant chemotherapy for muscle-invasive bladder cancer: Underused across the 49(th) parallel. Can Urol Assoc J. 2019;13(2):29-31. Epub 2019/02/06. https://doi.org/10.5489/cuaj.5827. PMID: 30721125
- Koshkin VS, Grivas P. Perioperative chemotherapy for muscle-invasive bladder cancer: the importance of multidisciplinary management for evidence-based practice and transformative research. Transl Androl Urol. 2018;7(3):504-7. Epub 2018/07/28. https://doi.org/10.21037/tau.2018.06.03. PMID: 30050808
- Advanced Bladder Cancer Meta-analysis Collaborators G. Adjuvant Chemotherapy for Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis of Individual Participant Data from Randomised Controlled Trials. Eur Urol. 2022;81(1):50-61. Epub 2021/11/23. https://doi.org/10.1016/j.eururo.2021.09.028. PMID: 34802798
- Donat SM, Shabsigh A, Savage C, Cronin AM, Bochner BH, Dalbagni G, et al. Potential impact of postoperative early complications on the timing of adjuvant chemotherapy in patients undergoing radical cystectomy: a high-volume tertiary cancer center experience. Eur Urol. 2009;55(1):177-85. Epub 2008/07/22. https://doi.org/10.1016/j.eururo.2008.07.018. PMID: 18640770
- McFerrin C, Davaro F, May A, Raza S, Siddiqui S, Hamilton Z. Trends in utilization of neoadjuvant and adjuvant chemotherapy for muscle invasive bladder cancer. Investig Clin Urol. 2020;61(6):565-72. Epub 2020/09/29. https://doi.org/10.4111/icu.20200132. PMID: 32985142
- Millar JL, Frydenberg M, Toner G, Syme R, Thursfield V, Giles GG, et al. Management of muscle-invasive bladder cancer in Victoria, 1990-1995. ANZ J Surg. 2006;76(3):113-9. Epub 2006/04/22. https://doi.org/10.1111/j.1445-2197.2006.03665.x. PMID: 16626343
- Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, Oh WK, et al. Treatment of patients with metastatic urothelial cancer "unfit" for Cisplatin-based chemotherapy. J Clin Oncol. 2011;29(17):2432-8. Epub 2011/05/11. https://doi.org/10.1200/JCO.2011.34.8433. PMID: 21555688
- Dall'Era MA, Cheng L, Pan CX. Contemporary management of muscle-invasive bladder cancer. Expert Rev Anticancer Ther. 2012;12(7):941-50. Epub 2012/08/01. https://doi.org/10.1586/era.12.60. PMID: 22845409
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-47. Epub 2008/12/23. https://doi.org/10.1016/j.ejca.2008.10.026. PMID: 19097774
- Booth CM, Siemens DR, Li G, Peng Y, Tannock IF, Kong W, et al. Perioperative chemotherapy for muscle-invasive bladder cancer: A population-based outcomes study. Cancer. 2014;120(11):1630-8. Epub 2014/04/16. https://doi.org/10.1002/cncr.28510. PMID: 24733278
- David KA, Milowsky MI, Ritchey J, Carroll PR, Nanus DM. Low incidence of perioperative chemotherapy for stage III bladder cancer 1998 to 2003: a report from the National Cancer Data Base. J Urol. 2007;178(2):451-4. Epub 2007/06/15. https://doi.org/10.1016/j.juro.2007.03.101. PMID: 17561135
- Macleod LC, Yabes JG, Yu M, Fam MM, Hale NE, Turner RM, 2nd, et al. Trends and appropriateness of perioperative chemotherapy for muscle-invasive bladder cancer. Urol Oncol. 2019;37(7):462-9. Epub 2019/05/06. https://doi.org/10.1016/j.urolonc.2019.04.006. PMID: 31053530
- Lu Z, Clement JM, Pan Q, Swede H, Mehta R, Wang X. Patterns and predictors of treatment in muscle-invasive bladder cancer (MIBC): A real-world study. Journal of Clinical Oncology. 2021;39(15_suppl):e16531-e.
- Walker M, Doiron RC, French SD, Brennan K, Feldman-Stewart D, Siemens DR, et al. Peri-Operative Chemotherapy for Bladder Cancer: A Survey of Providers to Determine Barriers and Enablers. Bladder Cancer. 2018;4(1):49-65. Epub 2018/02/13. https://doi.org/10.3233/BLC-170148. PMID: 29430507
- Boeri L, Soligo M, Frank I, Boorjian SA, Thompson RH, Tollefson M, et al. Delaying Radical Cystectomy After Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer is Associated with Adverse Survival Outcomes. Eur Urol Oncol. 2019;2(4):390-6. Epub 2019/07/07. https://doi.org/10.1016/j.euo.2018.09.004. PMID: 31277775
- Mmeje CO, Benson CR, Nogueras-Gonzalez GM, Jayaratna IS, Gao J, Siefker-Radtke AO, et al. Determining the optimal time for radical cystectomy after neoadjuvant chemotherapy. BJU Int. 2018;122(1):89-98. Epub 2018/03/24. https://doi.org/10.1111/bju.14211. PMID: 29569824
- Zargar H, Espiritu PN, Fairey AS, Mertens LS, Dinney CP, Mir MC, et al. Multicenter assessment of neoadjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol. 2015;67(2):241-9. Epub 2014/09/27. https://doi.org/10.1016/j.eururo.2014.09.007. PMID: 25257030
- Lee HW, Kwon WA, Nguyen NT, Phan DTT, Seo HK. Approaches to Clinical Complete Response after Neoadjuvant Chemotherapy in Muscle-Invasive Bladder Cancer: Possibilities and Limitations. Cancers (Basel). 2023;15(4). Epub 2023/02/26. https://doi.org/10.3390/cancers15041323. PMID: 36831665
- Culp SH, Dickstein RJ, Grossman HB, Pretzsch SM, Porten S, Daneshmand S, et al. Refining patient selection for neoadjuvant chemotherapy before radical cystectomy. J Urol. 2014;191(1):40-7. Epub 2013/08/06. https://doi.org/10.1016/j.juro.2013.07.061. PMID: 23911605
- Buttigliero C, Tucci M, Vignani F, Scagliotti GV, Di Maio M. Molecular biomarkers to predict response to neoadjuvant chemotherapy for bladder cancer. Cancer Treat Rev. 2017;54:1-9. Epub 2017/01/31. https://doi.org/10.1016/j.ctrv.2017.01.002. PMID: 28135623
- Choi SY, Ha MS, Chi BH, Kim JW, Chang IH, Kim TH, et al. Neoadjuvant versus adjuvant chemotherapy in bladder cancer: a nationwide cohort study. J Cancer Res Clin Oncol. 2022;148(11):3135-44. Epub 2022/01/22. https://doi.org/10.1007/s00432-022-03926-1. PMID: 35061097
- Nadal R, Apolo AB. Overview of Current and Future Adjuvant Therapy for Muscle-Invasive Urothelial Carcinoma. Curr Treat Options Oncol. 2018;19(7):36. Epub 2018/05/29. https://doi.org/10.1007/s11864-018-0551-z. PMID: 29808294
- Leow JJ, Martin-Doyle W, Rajagopal PS, Patel CG, Anderson EM, Rothman AT, et al. Adjuvant chemotherapy for invasive bladder cancer: a 2013 updated systematic review and meta-analysis of randomized trials. Eur Urol. 2014;66(1):42-54. Epub 2013/09/11. https://doi.org/10.1016/j.eururo.2013.08.033. PMID: 24018020