
Download

Bladder | 2022 | Vol. 9 | e47
DOI: 10.14440/bladder.2022.847
DOI: 10.14440/bladder.2022.847
REVIEW
Chinese botulinum toxin A for the treatment of lower urinary tract dysfunction: It works just as well
Fan Zhang1,‡, Qinggang Liu2,3,‡, Limin Liao1,2,3*, Xiaojuan Li4, Xueping Zhang4
1Department of Urology, China Rehabilitation Research Center, School of Rehabilitation Medicine, Capital Medical University, Beijing 100068, China
2Cheeloo College of Medicine, Shandong University, Jinan, Shandong 250012, China
3University of Health and Rehabilitation Sciences, Qingdao, Shandong 266000, China
4Lanzhou Institute of Biological Products, Lanzhou, Gansu 730046, China
2Cheeloo College of Medicine, Shandong University, Jinan, Shandong 250012, China
3University of Health and Rehabilitation Sciences, Qingdao, Shandong 266000, China
4Lanzhou Institute of Biological Products, Lanzhou, Gansu 730046, China
‡These two authors contributed equally to this article.
*Corresponding author: Limin Liao, Department of Urology, China Rehabilitation Research Center, Jiaomen North Road 10, Fengtai District, Beijing 100068, China, E-mail: lmliao@263.net
Conflict of interest: Authors declared no conflict of interest.
Abbreviations: BoNT/A, botulinum neurotoxin type A; LUTD, lower urinary tract dysfunction; SCI, spinal cord injury; OAB, overactive bladder; DSD, detrusor sphincter dyssynergia; NDO, neurogenic detrusor overactivity; IDO, idiopathic detrusor overactivity; IC/BPS, interstitial cystitis/bladder pain syndrome; UTI, urinary tract infection; BPH, benign prostatic hyperplasia; CPP, chronic prostatic pain; NAP, neurotoxin-associated proteins; PTC, progenitor toxin complex; EAU, European Association of Urology; API, active pharmaceutical ingredient; NT, neurotoxin; HA, hemagglutinin; NTNH, nontoxic non-HA; HPLC, high performance liquid chromatography; MTD, maximum tolerated dose; LD, lethal dose; NOAEL, no-observed-adverse-effect level; VUR, vesicoureteral reflux; PVR, postvoid residual; DO, detrusor overactivity; LUT, lower urinary tract; RV, reflex volume; ICS, International Continence Society; IC, intermittent catheterization; MCC, maximum cystometric capacity; MDP, maximum detrusor pressure; OABSS, overactive bladder symptom score; QoL, quality of life. AEs, adverse events; IHC, immunohistochemical; IPSS, international prostate symptom score; PSA, prostate specific antigen
Received October 28, 2021; Revision received March 7, 2022; Accepted March 22, 2022; Published September 14, 2022
Abstract
The botulinum neurotoxin type A (BoNT/A) is a neurotoxin produced by Clostridium botulinum. It causes botulism and represents the most powerful natural poison. In urological practice, the indications for BoNT/A therapy include neurogenic detrusor overactivity (NDO), idiopathic overactive bladder (OAB) or idiopathic detrusor overactivity (IDO), detrusor-sphincter dyssynergia (DSD), interstitial cystitis/bladder pain syndrome (IC/BPS), urinary tract infections (UTI), benign prostatic hyperplasia (BPH), and, more recently, chronic prostatic pain (CPP). BoNT/A is not only conducive to the treatment of muscle spasticity but also effectively works on hyperalgesia associated with various disorders of the lower urinary tract, thanks to its anti-nociceptive properties. While Botox® (Allergan Inc., Irvine, CA) is currently being used across the globe, we have been using Chinese BoNT/A for many years for the treatment of DSD, NDO, idiopathic OAB, IC/BPS, BPH and UTI. Our experience showed that Chinese BoNT/A was as good as other BoNT/A products in terms of efficacy, safety, and tolerability. In this study, we explored the current and potential applications of Chinese BoNT/A in urology, and reviewed the background information regarding the toxin.
Keywords: Botulinum neurotoxin type A; Hengli®; Lower urinary tract dysfunction; Detrusor overactivity; Bladder hyperalgesia
INTRODUCTION
Botulinum neurotoxin (BoNT), produced by Clostridium botulinum, is the most potent natural poison. When injected intramuscularly in minute quantities, this substance produces selective and reversible muscle weakness that persists for several months. In various medical fields, the toxin has been employed as a means of treating muscular hypercontraction [1]. BoNTs come in seven major serotypes (A-G) that are produced, in bacteria, along with non-toxic neurotoxin-associated proteins (NAPs) in the form of the progenitor toxin complex (PTC) [2,3]. Despite some differences in amino acid sequences, these serotypes all share a common basic structure. BoNTs differ biochemically with different types and among formulations of the same serotype. These distinctions might lead to discrepancies in therapeutic profiles (dose, efficacy, duration, safety) of the various toxins. Therefore, caution should be exercised when clinically comparing these indices among the toxins [4].
Botulinum neurotoxin type A (BoNT/A) is the major culprit of human botulism, and is the most widely used BoNT in clinical practice [5]. The BoNT/A is produced and marketed by several companies, with several formulations available. Many studies have been conducted involving Botox® (Allergan, Inc., Irvine, USA) and Dysport® (Ipsen, Inc., Slough, UK) in treating neurogenic detrusor overactivity (NDO). Other types A serotypes commercially available include Xeomin® (Merz Pharmaceuticals UK Ltd, Frankfurt am Main, Germany), Hengli® (Lanzhou Institute of Biological Products Ltd, Gansu, China), and PurTox® (Mentor Corporation, Santa Barbara, CA). These toxins all have a different non-proprietary name. Botox® and Dysport®, for instance, are also known as onabotulinumtoxinA and abobotulinumtoxinA, respectively. BoNT/A products are produced through different biological manufacturing processes, are obtained through different isolation and purification methods, and are drawn from different Clostridium batches.
Urological application of BoNT/A dates back to the 1980s when it was first used for the treatment of detrusor sphincter dyssynergia (DSD) [6]. A decade later, it was employed for treating idiopathic and neuropathic detrusor overactivity (IDO/NDO) [7]. Since BoNT/A is believed to temporarily block the presynaptic release of acetylcholine and, consequently, cause paralysis of detrusor smooth muscle, it is currently used as a second-line agent for the management of IDO and NDO. In the cases where anti-cholinergic medications are inadequate or intolerable, this treatment option appears to be a valuable alternative to surgery. It has been recommended by the European Association of Urology (EAU) and awarded a Grade A recommendation on the basis of its efficacy [4,8-9]. Nonetheless, the mechanism of the toxin appears more complicated than initially thought, and it might work on both motor and sensory nerves of the bladder. A wide array of lower urinary tract dysfunctions reportedly responded well to the agent. In this review, we focused on the biological and chemical properties of Chinese BoNT/A product and discussed the preclinical and clinical efficacy and safety of Chinese BoNT/A. Moreover, we shared our experience, with our readers, in the use of Chinese BoNT/A for the treatment of the lower urinary tract dysfunction (LUTD) over the last twenty years and present our results to demonstrate that Chinese BoNT/A is as effective as other BoNT/A products.
CHINESE BONT/A
Chinese BoNT/A is manufactured by Lanzhou Institute of Biological Products Ltd., Lanzhou, China. As a new drug, it was approved by the China Ministry of Health of China in 1993 and has been produced and marketed for more than 20 years. Hengli®, Prosigne®, and Lantox® are its trade names in China, Brazil, and Russian respectively. In light of its toxicity, stability, and ease of purification, Clostridium botulinum type A Hall strain has been utilized to produce Chinese BoNT/A. Nucleotide sequence comparison among samples (Master seed lot and working seed lot) and Hall strain of Clostridium BoNT/A stored in gene bank (No. AF488749) found that the homology of the two strains is more than 99% [10]. Therefore, we are led to concluded that the tested sample was Clostridium BoNT/A Hall strain, and the result showed that that Clostridium BoNT/A Hall strain and BoNT/A gene were very stable when stored for a long period of time. Chinese Lantox® and Allergan's Botox® appeared to have comparable efficacy, safety, tolerability, and dose profiles for the treatment of blepharospasm, hemifacial spasm, and cervical dystonia [11,12].
Active pharmaceutical ingredient (API)
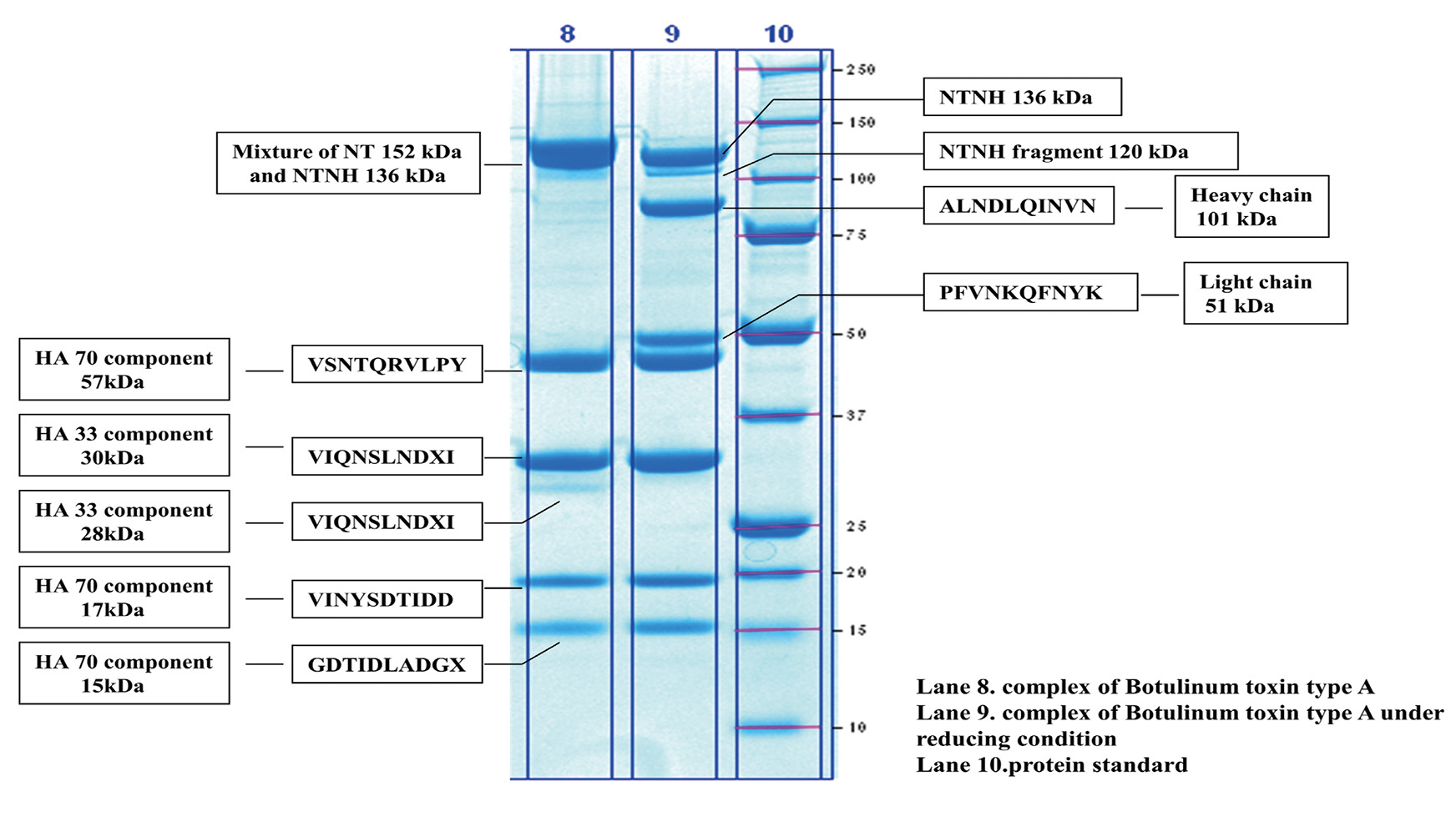
The active pharmaceutical ingredient (API) of Hengli® is crystalline BoNT/A (in complex form), which is composed of neurotoxin (NT), hemagglutinin (HA), and non-toxic non-HA (NTNH) linked through non-covalent bond. The high-performance liquid chromatography (HPLC) in 5 batches of the complex revealed only one peak, with the purity being over 99.5%. The integration of HPLC showed that the molecular mass of neurotoxin was about 150 kDa (R = 0.9944), indicating that it was highly pure. The mean specific activity of 24 batches of bulk of Hengli® manufactured in 2009–2011 was 3.0×107 LD50/mg protein (CV ≤ 2 SD), exceeding the standards of Chinese Pharmacopoeia and the European Pharmacopoeia (1.0×107 LD50/mg protein) [13]. SDS-PAGE of the complex exhibited the following bands: neurotoxin (152 kDa), NTNH (136 kDa, 120 kDa), HA70 component (57 kDa, 17 kDa, 15 kDa), and HA33 component (30 kDa and 28 kDa) (Fig. 1). However, HA17 was not detected and had been thought to be a component of the complex [5,14]. A reducing condition led to the neurotoxin being fragmented into two parts: a heavy chain (101 kDa) and a light chain (51 kDa), and the HA33 component (28 kDa) was cleaved as well (Fig. 1). This conclusion was further confirmed by N-terminal sequencing (NTNH was not detected in SDS-PAGE due to the small distance between the protein and the neurotoxin). Figure 2 shows a purified neurotoxin. This complex has an isoelectric point of 4.97. The API in Hengli® final product contains about 5 ng of protein per vial (100 U) based on the mean specific activity of bulks (3.0×107 LD50/mg protein), which indicates that a small amount of protein confers clinical benefits while posing a low risk of stimulating the patient’s immune system.
Other characteristics
Non-clinical pharmacokinetics
Presented here are the dynamics, distribution, intra-muscular diffusion, and excretion of Hengli® using Na125I radio-labeled BoNT/A in Wistar rats. Radiation diffusion studies showed that the 125I radio-labeled BoNT/A molecule did not cross the blood-brain barrier and was not found in the central nervous system. According to tissue diffusion studies, the BoNT/A complex remained concentrated at the intra-muscular site, with diffusion into the tissues over a distance of up to 0.25 cm. Toxin excretion studies showed that the toxin was mostly excreted into the urine and little was through the feces.
Pre-clinical safety study
The maximum tolerated dose (MTD) of Hengli® after an intramuscular injection into mice was 20 U/kg. The lethal dose (LD) for repeated intramuscular administration was approximately 40 U/kg, while the no-observed-adverse-effect level (NOAEL) was 16 U/kg. Consequently, for an adult (weighing 70 kg on average), the MTD, LD, and NOAEL for a single intramuscular injection are estimated to be 1400 U, 2800 U, and 1100 U, respectively. Since the normal therapeutic dose of Hengli® is significantly lower than its NOAEL, Hengli® is generally considered to be safe when used clinically.
Antigenicity and hemolytic activity
Our test on the antigenicity of Hengli® in four repeated-dose animal models failed to detect antibodies against active BoNT/A. At the 100 U/mL of Hengli®, no hemolysis or hemagglutination was observed in an in vitro study with rabbit erythrocytes [15].
Figure 1. SDS-PAGE analysis and N-terminal sequence test of complex of Chinese BoNT/A. BoNT/A: botulinum neurotoxin type A [15].
Figure 2. SDS-PAGE analysis and N-terminal sequence test of neurotoxin of Chinese BoNT/A. BoNT/A: botulinum neurotoxin type A [15].
MECHANISM OF ACTION
Botulinum toxin inhibits acetylcholine release at the neuromuscular junction and in sympathetic and parasympathetic neurons. It suppresses the transmission of alpha motor neurons at the neuromuscular junction, thereby resulting in weakness in striated muscles. In both smooth muscles and striated muscles, BoNT/A is internalized by pre-synaptic neurons upon its interaction with an extracellular receptor (gangliosides and possibly synaptic vesicle protein 2C). Cleavage of SNAP-25 in the synaptic fusion complex of neurons enables BoNT/A to disrupt the fusion between the acetylcholine-containing vesicles and the membrane of neurons. This results in selective paralysis of the low-grade contractions of the detrusor overactivity, while still allowing for high-grade contractions that initiate micturition. Additionally, BoNT/A modulates afferent nerve activity by inhibiting the release of substance P, calcitonin gene-related peptides, and glutamate from afferent nerves, and by reducing the level of nerve growth factor. This effect on sensory feedback loops may not only explain the mechanism by which BoNT/A relieves overactive bladder (OAB) but may also help us gain insight into its role in relieving hyperalgesia, which is associated with lower urinary tract disorders [16].
INJECTION PROTOCOL IN UROLOGICAL PRACTICE
In virtually all studies using BoNT/A, BoNT/A was directly injected into the detrusor. Several studies utilized the suburothelial injection to take advantage of the presumed effect on afferent sensory nerves [17]. While most studies reported sparing the trigone because of possible effects on vesicoureteral reflux (VUR), two studies injected it into the trigone without reporting VUR [18,19].
Other variables of the protocol include the type of cystoscopy and the anesthesia. No study compared the efficacy or tolerability of BoNT/A injections with rigid or flexible cystoscope. Even though both flexible and rigid cystoscopes have been employed (including our center), rigid ones were more commonly used. The flexible cystoscopy, however, presents a distinct advantage for men with preserved sensibility or, regardless of gender, for patients with SCI with a lesion above the T6, since reduced pain or stimulation prevents autonomic dysreflexia. Various types of anesthesia, including local, spinal, and general ones, have been used during Botox injections. In our opinion, the choice of anesthesia is up to the patient and surgeon, mainly depending on bladder and urethral sensation. According to our experience, intravenous general anesthesia is easy to perform and might be a suitable option for patients having high-level anxiety or sensitivity or for those who are at risk for autonomic dysreflexia.
UROLGOICAL APPLICATIONS OF CHINESE BONT/A
Various BoNT/A products have been studied with respect to their effects on LUTD diseases, including DSD, NDO, idiopathic OAB, IC/BPS, BPH and UTI, and their effect on quality of life [20]. Here, we present our experience in using Chinese BoNT/A for the treatment of LUTD diseases over the past twenty years and the results are summarized in Table 1.
BoNT/A and detrusor-sphincter dyssynergia (DSD)
In patients with SCI, DSD is a major cause of morbidity. By urethral sphincter injection of BoNT/A, Dykstra et al., for the first time, described a reversible chemical sphincterotomy and a reduction in DSD in SCI patients [6]. Alternatively, BoNT/A has been injected transurethrally using a cystoscope or transperineally under electromyographic control. An injection of 140 units of toxin was given transurethrally via a cystoscope to achieve the best result. A subsequent dose of 240 units was administered weekly. The maximum reduction in post-void residual volume (PVR) was attained upon an average of three injections. The effect lasted for approximately 50 days. These results suggest that BoNT/A injections into the external urethral sphincter are effective in treating DSD in people with SCI. To maintain efficacy of the treatment, re-injection is required. However, large randomized studies comparing the effects of this treatment with a placebo are still lacking.
A study at our center assessed the effect of 200 units of Hengli® injection into the urinary sphincter for the treatment of DSD in 19 patients with SCI and hydronephrosis. Results showed that it could effectively decrease urethral pressure, detrusor leak point pressure, and PVR in SCI patients. A significant improvement in PVR was observed 9.5 days after operation and persisted for 3.8 months on average. It is an effective, minimally-invasive, safe, reversible, repeatable option for treating DSD as well as retaining upper urinary tract function [21].
BoNT/A and neurogenic / idiopathic detrusor overactivity (NDO/IDO)
Detrusor overactivity (DO) is a urodynamic state characterized by involuntary detrusor contractions during the filling phase, which may be spontaneous or provoked according to the standardization of terminology for lower urinary tract (LUT) function published by the International Continence Society (ICS) [22]. NDO is diagnosed when there exists a relevant underlying neurologic condition (e.g., spinal cord injury or multiple sclerosis). Anti-muscarinic drugs are commonly prescribed as first-line therapies for patients with NDO. However, they can be ineffective in some patients or cause intolerable side effects, such as dry mouth, constipation, and blurred vision. The injection of BoNT/A into the bladder wall shows promise in treating intractable OAB syndrome with either neurogenic or idiopathic causes [23].
Table 1. Clinical applications of Chinese botulinum toxin A for lower urinary tract dysfunction
| LUTD | Therapeutic effects | Target | Dose used | References |
|---|---|---|---|---|
| DSD | Decreased urethral pressure, detrusor leak point pressure, and PVR | External urethral sphincter | 200 U | [21] |
| NDO | Improved continence, increased bladder capacity, improved PVR, RV, MCC, and MDP | Detrusor | 300 U | [27-30] |
| OAB/IDO | Improved micturition frequency, urgency, and OABSS | Detrusor | 100 U | [35] |
| IC/BPS | Reduced bladder pain and urinary frequency, and increased QoL | Detrusor and suburothelium (trigone) | 100U | [41] |
| UTI | Reduced UTI significantly in SCI patients with NDO, decreased maximum detrusor pressure | Detrusor | 300U | [53] |
LUTD: lower urinary tract dysfunction; SCI: spinal cord injury; DSD: detrusor sphincter dyssynergia; NDO: neurogenic detrusor overactivity; IDO: idiopathic detrusor overactivity; IC/BPS: interstitial cystitis/bladder pain syndrome; UTI: urinary tract infection; PVR: postvoid residual; RV: reflex volume; MCC: maximum cystometric capacity; MDP: maximum detrusor pressure; OABSS: overactive bladder symptom score; QoL: quality of life.
Schurch et al. reported that injecting BoNT/A into the detrusor muscle of SCI patients had a therapeutic effect in a non-randomized prospective study [24,25]. Upon successful treatment, the patient becomes continent and may withdraw or decrease their intake of anticholinergic drugs. BoNT/A causes bladder paresis that will remain for at least nine months, and after this repeated injections are required. This trial was based on the hypothesis that BoNT/A may block parasympathetic action as proposed by Dickson and Shevky [26].
Over the past decades, we have been using this procedure with Hengli® [27-30]. The data of our institution principally covered the time frame from 2002 to 2005 in 78 SCI patients and found that repeated Hengli® injections into the detrusor were efficatious, safe, feasible, and minimally-invasive for the treatment of DO and neurogenic incontinence. After the first injection, the mean frequency of incontinence decreased from 13.5 to 2.7 times, and the mean volume of intermittent catheterization (IC) increased from 131 mL to 389 mL each time. The average time to efficacy was 7.6 days. Among 10 patients who received a second injection 8.9 months after the first one, the frequency of incontinence decreased from 9.7 to 3.7 times per day, and the volume of IC increased from 108 mL to 387 mL. In 6 patients, the third injection was given 5.8 months after the second injection, and the mean frequency of incontinence declined from 9.2 to 3.9 times per day, while IC volume increased from 116 mL to 364 mL. Our retrospective study between 2002 and 2009 found that the bladder function improved significantly, along with continence and subjective satisfaction in 108 SCI patients [27]. In this study, the patients accomplished significant clinical and urodynamic improvements after 6 months. Nineteen patients were treated with repeated Hengli® injections and the maximum number of injections was five. Against the baseline, PVR, reflex volume (RV), maximum cystometric capacity (MCC), and maximum detrusor pressure (MDP) all improved significantly after each Hengli® injection.
According to a comparative study between IDO and NDO patients, both IDO and NDO patients showed equally beneficial effect in short-term in terms of urgency, frequency, and urgency incontinence episodes [31]. Symptomatic improvement is one of the early signs of a patient's clinical response to BoNT/A, generally reported within one week after treatment [32]. Up to 16 weeks after treatment, intra-detrusor BoNT/A injections resulted in significant, comparable improvements in patients with refractory DO of either neurogenic or idiopathic origin. Post-treatment changes in the quality of life (QoL) were correlated with changes in LUT symptoms, but not with respective changes in urodynamic parameters [33]. We conducted a multi-center, prospective, randomized, double-blind, placebo-controlled trial, which evaluated the efficacy and safety of Hengli® for the treatment of IDO. The results showed that 100 U Hengli® was well-tolerated and attained significant improvements in OAB symptoms in Chinese patients who had been inadequately managed by anticholinergics. Significant differences in micturition frequency and urgency episodes were already observed at Week 2 post-treatment as compared to the placebo group. Adverse events (AEs) associated with the Hengli® treatment included increased PVR, dysuria, and UTIs. All AEs were mild or moderate. The findings of this trial with Hengli® BoNT/A were consistent with the results of other studies that found Botox® treatment did improve OAB symptoms [34,35].
BoNT/A and interstitial cystitis/bladder pain syndrome (IC/BPS)
The pathophysiology of IC/BPS is not fully understood. Pain relief is currently the focus of IC/BPS management. Kuo et al. suggested that nerve growth factors were elevated in bladder tissue of IC patients but returned to normal after BoNT-A plus hydrodistension in responsive patients [36]. An immunohistochemical (IHC) study showed that chronic inflammation and apoptotic signaling molecules were significantly reduced after repeated BoNT/A injections in patients with IC/BPS. The improvement in IHC findings was correlated with clinical improvement [37]. In addition to examining the long-term effects of BoNT/A in IC patients, a series of 15 IC patients were followed up for 12 months after bladder injection with 200 U of BoNT/A [38]. After three months, 87% (13/15) of patients reported subjective improvement in a follow-up, along with significant reduction in visual analog scale scores, nocturia frequency, and daytime micturition frequency. By 5 months, only 27% of patients reported improvement in symptoms, and by 12 months, all patients reported return of bladder symptoms. Prior studies have shown that repeated BoNT/A injections were safe and effective for patients with IC/BPS and could achieve more favorable outcomes than a single injection [39,40].
Data from 124 female IC/BPS patients in our center from 2003 to 2013 were retrospectively analyzed [41]. Among these subjects, 66 received Hengli®, and 58 were given sodium hyaluronate (Cystistat) instillation along with bladder hydrodistension. A 100-unit intravesical injection of Hengli® was immediately followed by cystoscopic hydrodistention under intravenous general anesthesia. Patients were evaluated on the O'Leary-Sant scale, and the visual analog scale (VAS), in urination frequencies, and by a quality of life questionnaire. Results have shown that Hengli® was effective for up to 6 months following treatment. Hydrodistention plus cystistat remained effective for a period of 3 months after treatment, and 19.0% (11/58) of the subjects switched to Hengli® injections due to insufficient effects. About 34.8% (23/66) of the patients received repeated Hengli® injections. Repeated injections were well tolerated and effective. The maximal treatment course included four injection cycles. These results suggested that Hengli® injection was a safe and effective therapeutic option for patients with IC/BPS.
BoNT/A and the Prostate
BoNT/A injections into the external urethral sphincter have been shown to reduce chronic prostatic pain (CPP), presumably by reducing sphincter hyperactivity [42]. In patients with chronic prostatitis/chronic pelvic pain syndrome, intraprostatic BoNT/A injections significantly relieved prostate pain and urination frequency. Furthermore, patients with CPP due to pelvic muscular pain and spasm benefit from localized BoNT/A injections [43]. Dyspareunia and pelvic floor pressure could be reduced by injecting BoNT/A into the pelvic floor muscle. BoNT/A was used off-label, for the first time, to treat BPH in humans by Maria et al. [44]. This randomized, placebo-controlled study involved 30 men with symptomatic BPH who were randomly assigned to receive either intraprostatic injections of saline or 200 units of Botox. The improvement in clinical symptoms was conspicuous within a month of treatment. After 2 months, 13 patients in the treatment group (87%), against 3 patients in the control group (10%), reported BPH symptom relief (P = 0.00001). At 12 months, the percent improvement, in terms of the international prostate symptom score (IPSS), Qmax, PVR, and prostate size, was 62%, 85%, 81%, and 61%, respectively. A 38% reduction in prostate specific antigen (PSA) values was also noted. The beneficial effect persisted for 12 months even after a single injection. No urinary incontinence or systemic side effects were reported over the 19.6-month follow-up period. Chuang et al. stratified patients who had failed medical treatment on the basis of prostate size: those with < 30 mL received 100 units of Botox® while those with > 30 mL received 200 units (perineal injection) [45]. After 12 months, IPSS, Qmax, and PVR showed similar improvements to those of Maria et al. (2003), except that the percent shrinkage of prostate size was much smaller (13–19% vs. 61%). In 12 of 41 men (29%), no change was found in prostate volume, although 7 of these 12 men (58%) experienced a greater than 30% reduction in IPSS, Qmax, and PVR, suggesting that BoNT/A might alleviate BPH symptoms not by reducing prostate size alone. Although the aforementioned studies have demonstrated the potential of BoNT/A for the treatment of BPH, other studies failed to consistently yield the same results [46,47]. In a placebo-controlled, randomized, double-blind, phase II trial, no significant improvement was observed in patients with LUTS and BPH who were treated with BoNT/A [48].
BoNT/A and urinary tract infection (UTI)
UTI is the major culprit of morbidity in neuropathic patients [49,50]. Patients with neurogenic lower urinary tract dysfunction are at greater risk of UTI when they have a VUR, a high bladder pressure, or an indwelling catheter [50,51]. NDO is still the most significant factor for the higher risk of UTI when patients receive intermittent catheterization since high bladder pressure increases the possibility of VUR. A prospective non-randomized study evaluated the incidence of UTI in 30 NDO patients after receiving 300 U of BoNT/A detrusor injections. Results showed a significant decrease in UTI over a period of time of 6 months (P = 0.003). The effect seems to be related to improved urodynamic parameters after injection (volume of the first uninhibited contraction, MDP, and MCC), which reflects enhanced reservoir capacity at low pressure [52].
A single-arm clinical trial at our center from 2010 to 2012 looked into the effects of Chinese BoNT/A injections into detrusor on UTIs in patients with spinal cord injury [53]. UTI was defined as a colony count of 105 colony-forming units per milliliter or more, with a fever over 38°C and two of the following symptoms, i.e., uncomfortable distention of the bladder, lower abdominal pain, increased urinary incontinence, increased spasticity, autonomic hyperreflexia, and increased sweating or malaise. The results showed that Hengli® detrusor injection reduced UTI significantly in SCI patients with NDO. A decrease in detrusor pressure is thought to be responsible for this effect [53].
CONCLUSIONS
The BoNT/A is emerging as a valuable alternative for the treatment of a variety of disorders, and has been used as the treatment of choice for some conditions. DSD, NDO, urinary incontinence, OAB, and CPP are urological conditions that are often refractory to currently-available treatments and may respond to BoNT/A therapy. Many questions remain about the effect of BoNT/A on neural pathways that modulate the LUT. Our study demonstrated that Chinese version of BoNT/A exhibited similar efficacy, safety, and tolerability to other BoNT/A products for the treatment of lower urinary tract dysfunction and other disorders.
Source of Funding
This study was supported by a grant from Chinese National Natural Science Foundation (No. 81870523).
Author Contributions
F.Z., Q.G.L., L.M.L. wrote this manuscript; F.Z., Q.G.L., X.J.L. and X.P.Z. prepared the draft; L.M.L. outlined and revised the manuscript; all authors read and approved the final manuscript.
References
- Munchau A, Bhatia KP. Uses of botulinum toxin injection in medicine today. BMJ. 2000 Jan 15;320(7228):161-5. https://doi.org/10.1136/bmj.320.7228.161 PMID: 10634738
- Dover N, Barash JR, Hill KK, Xie G, Arnon SS. Molecular characterization of a novel botulinum neurotoxin type H gene. J Infect Dis. 2014 Jan 15;209(2):192-202. https://doi.org/10.1093/infdis/jit450 PMID: 24106295
- Hill KK, Smith TJ. Genetic diversity within Clostridium botulinum serotypes, botulinum neurotoxin gene clusters and toxin subtypes. Curr Top Microbiol Immunol. 2013;364:1-20. https://doi.org/10.1007/978-3-642-33570-9_1 PMID: 23239346
- Nitti VW. Botulinum toxin for the treatment of idiopathic and neurogenic overactive bladder: state of the art. Rev Urol. 2006 Fall;8(4):198-208. PMID: 17192799
- Yao G, Lee K, Gu S, Lam KH, Jin R. Botulinum neurotoxin A complex recognizes host carbohydrates through its hemagglutinin component. Toxins (Basel). 2014 Feb 12;6(2):624-35. https://doi.org/10.3390/toxins6020624 PMID: 24525478
- Dykstra DD, Sidi AA. Treatment of detrusor-sphincter dyssynergia with botulinum A toxin: a double-blind study. Arch Phys Med Rehabil. 1990 Jan;71(1):24-6. PMID: 2297305
- Stohrer M, Schurch B, Kramer G. Botulinum A-toxin in the treatment of detrusor hyperreflexia in spinal cord injured patients: a new alternative to medical and surgical procedures? J Urol. 2000 Sep;164(3 Pt 1):692-7. https://doi.org/10.1097/00005392-200009010-00018 PMID: 10953127
- Karsenty G, Denys P, Amarenco G, De Seze M, Gamé X, Haab F, et al. Botulinum toxin A (Botox) intradetrusor injections in adults with neurogenic detrusor overactivity/neurogenic overactive bladder: a systematic literature review. Eur Urol. 2008 Feb;53(2):275-87. https://doi.org/10.1016/j.eururo.2007.10.013 PMID: 17988791
- Leippold T, Reitz A, Schurch B. Botulinum toxin as a new therapy option for voiding disorders: current state of the art. Eur Urol. 2003 Aug;44(2):165-74. https://doi.org/10.1016/s0302-2838(03)00250-1 PMID: 12875934
- Zhao Y, Wei R, Liu CM, Zhang XP, Feng DJ, Gao XJ, et al. [Cloning and Sequencing of Complete BoNT Gene of Clostridium botulinum Type A for Therapy]. Chin J Biologicals. 2010;23(06):598-601. Chinese. https://doi.org/10.13200/j.cjb.2010.06.43.zhaoyj.010.
- Quagliato EM, Carelli EF, Viana MA. Prospective, randomized, double-blind study, comparing botulinum toxins type a botox and prosigne for blepharospasm and hemifacial spasm treatment. Clin Neuropharmacol. 2010 Jan-Feb;33(1):27-31. https://doi.org/10.1097/WNF.0b013e3181c46f61 PMID: 20124784
- Rieder CR, Schestatsky P, Socal MP, Monte TL, Fricke D, Costa J, et al. A double-blind, randomized, crossover study of prosigne versus botox in patients with blepharospasm and hemifacial spasm. Clin Neuropharmacol. 2007 Jan-Feb;30(1):39-42. https://doi.org/10.1097/01.Wnf.0000236771.77021.3c PMID: 17272968
- He X, Miao CH, Li XJ, Wang YT, Liang Q, Zhang XP, et al. [Biological characteristics and quality of botulinum toxin type A for injection]. Chin J Biologicals. 2012;25(11):1488-91, 97. Chinese. https://doi.org/10.13200/j.cjb.2012.11.89.hex.039.
- Inoue K, Fujinaga Y, Watanabe T, Ohyama T, Takeshi K, Moriishi K, et al. Molecular composition of Clostridium botulinum type A progenitor toxins. Infect Immun. 1996;64(5):1589-94. https://doi.org/10.1128/iai.64.5.1589-1594.1996 PMID: 8613365
- Liang Q, Chen S, Zhang R, Wei Z, Su J, Zhou Y, et al. [Nonclinical safety evaluation of botulinum toxin type A and botulinum neurotoxin type A]. Chin J Biologicals. 2017;30(07):710-7. Chinese. https://doi.org/10.13200/j.cnki.cjb.001797.
- Chapple C, Patel A. Botulinum toxin--new mechanisms, new therapeutic directions? Eur Urol. 2006;49(4):606-8. https://doi.org/10.1016/j.eururo.2006.01.005 PMID: 16457945
- Kuo HC. Therapeutic effects of suburothelial injection of botulinum a toxin for neurogenic detrusor overactivity due to chronic cerebrovascular accident and spinal cord lesions. Urology. 2006;67(2):232-6. https://doi.org/10.1016/j.urology.2005.08.016 PMID: 16442605
- Schulte-Baukloh H, Schobert J, Stolze T, Stürzebecher B, Weiss C, Knispel HH. Efficacy of botulinum-A toxin bladder injections for the treatment of neurogenic detrusor overactivity in multiple sclerosis patients: an objective and subjective analysis. Neurourol Urodyn. 2006;25(2):110-5. https://doi.org/10.1002/nau.20153 PMID: 16470519
- Smith CP, Nishiguchi J, O'Leary M, Yoshimura N, Chancellor MB. Single-institution experience in 110 patients with botulinum toxin A injection into bladder or urethra. Urology. 2005;65(1):37-41. https://doi.org/10.1016/j.urology.2004.08.016 PMID: 15667859
- Jiang YH, Liao CH, Kuo HC. Current and potential urological applications of botulinum toxin A. Nat Rev Urol. 2015;12(9):519-33. https://doi.org/10.1038/nrurol.2015.193 PMID: 26260879
- Liao L, Fu G, Shi WB, Xiong ZS, Ju YH, Wu J, et al. [Botulinum-A toxin injection in urinary sphincter by endoscope to treat detrusor-sphincter dyssynergia in patients with spinal cord injury]. Chin J Spine and Spinal Cord. 2006;(06):409-12. Chinese. https://doi.org/10.3969/j.issn.1004-406X.2006.06.002
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61(1):37-49. https://doi.org/10.1016/s0090-4295(02)02243-4 PMID: 12559262
- Sahai A, Khan M, Fowler CJ, Dasgupta P. Botulinum toxin for the treatment of lower urinary tract symptoms: a review. Neurourol Urodyn. 2005;24(1):2-12. https://doi.org/10.1002/nau.20090 PMID: 15578628
- Schurch B, Schmid DM, Stöhrer M. Treatment of neurogenic incontinence with botulinum toxin A. N Engl J Med. 2000;342(9):665. https://doi.org/10.1056/nejm200003023420918 PMID: 10702067
- Schurch B, Stöhrer M, Kramer G, Schmid DM, Gaul G, Hauri D. Botulinum-A toxin for treating detrusor hyperreflexia in spinal cord injured patients: a new alternative to anticholinergic drugs? Preliminary results. J Urol. 2000 Sep;164(3 Pt 1):692-7. https://doi.org/10.1097/00005392-200009010-00018 PMID: 10953127
- Dickson EC, Shevky R. Botulism. Studies on the manner in which the toxin of clostridium botulinum acts upon the body: I. The effect upon the autonomic nervous system. J Exp Med. 1923 Apr 30;37(5):711-31. https://doi.org/10.1084/jem.37.5.711 PMID: 1986875
- Chen G, Liao L. Injections of Botulinum Toxin A into the detrusor to treat neurogenic detrusor overactivity secondary to spinal cord injury. Int Urol Nephrol. 2011 Sep;43(3):655-62. https://doi.org/10.1007/s11255-010-9873-x PMID: 21110094
- Li D, Liao L, Xiong ZS, Fu G, Ju YH, Wu J, et al. [Botulinum toxin type A repeated injections into detrusor to treat detrusor hyperreflexia and neurogenic incontinence in spinal cord injury patients: 6 cases report]. Chin J Rehabil Theory Practice. 2005;(11):30-1. Chinese. https://doi.org/10.3969/j.issn.1006-9771.2005.11.01229.
- Liao L, Li D, Xiong ZS, Han CS, Huang Y, Shi WB. [Botulinum-A toxin injection into detrusor to treat detrusor hyperreflexia and neurogenic incontinence in patients with spinal cord injury]. Chin J Urol. 2004;(09):19-21. Chinese. https://doi.org/10.3760/j:issn:1000-6702.2004.09.006
- Liao L, Ju Y, Li D. [Botulinum Toxin-A Injection into Detrusor to Treat Neurogenic Detrusor Overactivity in Patient s with Spinal Cord Injury]. Chin J Rehabil Theory Practice. 2007;(11):1014-6. Chinese. https://doi.org/10.3969/j.issn.1006-9771.2007.11.005
- Popat R, Apostolidis A, Kalsi V, Gonzales G, Fowler CJ, Dasgupta P. A comparison between the response of patients with idiopathic detrusor overactivity and neurogenic detrusor overactivity to the first intradetrusor injection of botulinum-A toxin. J Urol. 2005 Sep;174(3):984-9. https://doi.org/10.1097/01.ju.0000169480.43557.31 PMID: 16094019
- Rapp DE, Lucioni A, Katz EE, O'Connor RC, Gerber GS, Bales GT. Use of botulinum-A toxin for the treatment of refractory overactive bladder symptoms: an initial experience. Urology. 2004 Jun;63(6):1071-5. https://doi.org/10.1016/j.urology.2004.01.041 PMID: 15183952
- Kalsi V, Apostolidis A, Popat R, Gonzales G, Fowler CJ, Dasgupta P. Quality of life changes in patients with neurogenic versus idiopathic detrusor overactivity after intradetrusor injections of botulinum neurotoxin type A and correlations with lower urinary tract symptoms and urodynamic changes. Eur Urol. 2006 Mar;49(3):528-35. https://doi.org/10.1016/j.eururo.2005.12.012 PMID: 16426735
- Chapple C, Sievert KD, MacDiarmid S, Khullar V, Radziszewski P, Nardo C, et al. OnabotulinumtoxinA 100 U significantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence: a randomised, double-blind, placebo-controlled trial. Eur Urol. 2013 Aug;64(2):249-56. https://doi.org/10.1016/j.eururo.2013.04.001 PMID: 23608668
- Liao LM, Liu QG, Cong HL, Xu ZH, Li EH, Weng ZL, et al. Hengli® Chinese Botulinum Toxin Type A for Treatment of Patients With Overactive Bladder: A Multicenter, Prospective, Randomized, Double-Blind, Placebo-Controlled Trial. Front Pharmacol. 2022 Feb 18;13:840695. https://doi.org/10.3389/fphar.2022.840695 PMID: 35250586
- Liu HT, Kuo HC. Intravesical botulinum toxin A injections plus hydrodistension can reduce nerve growth factor production and control bladder pain in interstitial cystitis. Urology. 2007 Sep;70(3):463-8. https://doi.org/10.1016/j.urology.2007.04.038 PMID: 17905097
- Shie JH, Liu HT, Wang YS, Kuo HC. Immunohistochemical evidence suggests repeated intravesical application of botulinum toxin A injections may improve treatment efficacy of interstitial cystitis/bladder pain syndrome. BJU Int. 2013 Apr;111(4):638-46. https://doi.org/10.1111/j.1464-410X.2012.11466.x PMID: 22943596
- Giannantoni A, Porena M, Costantini E, Zucchi A, Mearini L, Mearini E. Botulinum A toxin intravesical injection in patients with painful bladder syndrome: 1-year followup. J Urol. 2008 Mar;179(3):1031-4. https://doi.org/10.1016/j.juro.2007.10.032 PMID: 18206941
- Kuo HC. Repeated intravesical onabotulinumtoxinA injections are effective in treatment of refractory interstitial cystitis/bladder pain syndrome. Int J Clin Pract. 2013 May;67(5):427-34. https://doi.org/10.1111/ijcp.12113 PMID: 23574103
- Kuo HC. Repeated onabotulinumtoxin-a injections provide better results than single injection in treatment of painful bladder syndrome. Pain Physician. 2013 Jan;16(1):E15-23. https://doi.org/10.36076/ppj.2013/16/e15 PMID: 23340540
- Gao Y, Liao L. Intravesical injection of botulinum toxin A for treatment of interstitial cystitis/bladder pain syndrome: 10 years of experience at a single center in China. Int Urogynecol J. 2015 Jul;26(7):1021-6. https://doi.org/10.1007/s00192-015-2631-y PMID: 25690160
- Zermann D, Ishigooka M, Schubert J, Schmidt RA. Perisphincteric injection of botulinum toxin type A. A treatment option for patients with chronic prostatic pain? Eur Urol. 2000 Oct;38(4):393-9. https://doi.org/10.1159/000020314 PMID: 11025376
- Jhang JF, Kuo HC. Novel Treatment of Chronic Bladder Pain Syndrome and Other Pelvic Pain Disorders by OnabotulinumtoxinA Injection. Toxins (Basel). 2015 Jun 18;7(6):2232-50. https://doi.org/10.3390/toxins7062232 PMID: 26094697
- Maria G, Brisinda G, Civello IM, Bentivoglio AR, Sganga G, Albanese A. Relief by botulinum toxin of voiding dysfunction due to benign prostatic hyperplasia: results of a randomized, placebo-controlled study. Urology. 2003 Aug;62(2):259-64; discussion 264-5. https://doi.org/10.1016/s0090-4295(03)00477-1 PMID: 12893330
- Chuang YC, Chiang PH, Yoshimura N, De Miguel F, Chancellor MB. Sustained beneficial effects of intraprostatic botulinum toxin type A on lower urinary tract symptoms and quality of life in men with benign prostatic hyperplasia. BJU Int. 2006 Nov;98(5):1033-7; discussion 337. https://doi.org/10.1111/j.1464-410X.2006.06479.x PMID: 16956361
- Kuo HC, Liu HT. Therapeutic effects of add-on botulinum toxin A on patients with large benign prostatic hyperplasia and unsatisfactory response to combined medical therapy. Scand J Urol Nephrol. 2009;43(3):206-11. https://doi.org/10.1080/00365590902811537 PMID: 19308807
- De Kort LM, Kok ET, Jonges TN, Rosier PF, Bosch JL. Urodynamic effects of transrectal intraprostatic Ona botulinum toxin A injections for symptomatic benign prostatic hyperplasia. Urology. 2012 Oct;80(4):889-93. https://doi.org/10.1016/j.urology.2012.06.004 PMID: 22854138
- Marberger M, Chartier-Kastler E, Egerdie B, Lee KS, Grosse J, Bugarin D, et al. A randomized double-blind placebo-controlled phase 2 dose-ranging study of onabotulinumtoxinA in men with benign prostatic hyperplasia. Eur Urol. 2013 Mar;63(3):496-503. https://doi.org/10.1016/j.eururo.2012.10.005 PMID: 23098762
- Soden RJ, Walsh J, Middleton JW, Craven ML, Rutkowski SB, Yeo JD. Causes of death after spinal cord injury. Spinal Cord. 2000 Oct;38(10):604-10. https://doi.org/10.1038/sj.sc.3101080 PMID: 11093321
- Whiteneck GG, Charlifue SW, Frankel HL, Fraser MH, Gardner BP, Gerhart KA, et al. Mortality, morbidity, and psychosocial outcomes of persons spinal cord injured more than 20 years ago. Paraplegia. 1992 Sep;30(9):617-30. https://doi.org/10.1038/sc.1992.124 PMID: 1408338
- Esclarín De Ruz A, García Leoni E, Herruzo Cabrera R. Epidemiology and risk factors for urinary tract infection in patients with spinal cord injury. J Urol. 2000 Oct;164(4):1285-9. PMID: 10992382
- Gamé X, Castel-Lacanal E, Bentaleb Y, Thiry-Escudié I, De Boissezon X, Malavaud B, et al. Botulinum toxin A detrusor injections in patients with neurogenic detrusor overactivity significantly decrease the incidence of symptomatic urinary tract infections. Eur Urol. 2008 Mar;53(3):613-8. https://doi.org/10.1016/j.eururo.2007.08.039 PMID: 17804150
- Jia C, Liao LM, Chen G, Sui Y. Detrusor botulinum toxin A injection significantly decreased urinary tract infection in patients with traumatic spinal cord injury. Spinal Cord. 2013 Jun;51(6):487-90. https://doi.org/10.1038/sc.2012.180 PMID: 23357928